




This is a republication of the paper below, under the title above.
The Availablists: Emergency Care without the Emergency Department
NEJM Catalyst
Judd E. Hollander, MD, FACEP and Rahul Sharma, MD, MBA, FACEP
December 21, 2021
Dr. Rahul Sharma. Credit: John Abbott
Summary
Emergency care providers have been the “availablists” for both life-threatening conditions and immediate care generally.
The Covid-19 pandemic has transformed our mindset and approach to emergency care.
The pandemic forced health system leaders to redesign all aspects of care delivery, including how to extend emergency care beyond the four walls of the emergency department.
Despite being the health care system’s safety net, emergency departments are universally stressed due to capacity, staffing, and resource limitations, and yet cannot routinely reduce or suspend service.
The authors discuss challenges within the current system, the core value of emergency medicine, and possible changes in emergency care models, some already used successfully during the pandemic, that they believe will define the future of emergency care.
Introduction
Covid-19 had an immediate effect on our health care system. Institutions that considered themselves successful by making incremental changes over years were forced to overhaul their operations overnight.
The traditional model of predominantly in-person care morphed into a virtual system within days. “Late adopters” were forced to become immediate adapters.
Simultaneously, emergency departments (ED) witnessed unprecedented declines in volume. In the months that followed the first peak of the pandemic, the decreased ED volume adversely affected employment for emergency physicians, resulting in reduction in hours and rescissions of fully executed employment offers.
While ED volume appears to be trending upwards, it remains to be seen if it will reach sustainable pre-Covid-19 levels.
These disrupters have created an ideal opportunity to develop new and alternative models of emergency care to provide comprehensive, high-quality, patient-centric health care.
These disrupters have created an ideal opportunity to develop new and alternative models of emergency care to provide comprehensive, high-quality, patient-centric health care.
Emergency Medicine Is at the Breaking Point
Emergency departments, designed to provide essential expertise for patients with time-sensitive conditions, are perpetually under stress. Patients often go the ED when they cannot get care elsewhere. Health systems often send patients to the ED when they cannot accommodate them elsewhere. The ED was not designed for these uses, and they tax its capacity, staffing, and resources, especially when it must also act as surge capacity for natural disasters, public health crises, and mass casualty attacks. Too many EDs are forced to function in a reactionary mode without a clear vision for both the patient and the health system.
The Institute of Medicine’s 2006 report, aptly named Hospital-Based Emergency Care: At the Breaking Point delineated these issues, and they have not gotten better. Emergency departments function as the safety net of health care and cannot reduce or suspend service for any length of time. In addition to treating trauma and stroke patients, EDs serve our most vulnerable populations, often acting as the sole point of care. This long-standing issue was addressed in a recent review in NEJM Catalyst, which examined the root causes of emergency department crowding, described its harmful impact, and reviewed the evidence supporting attempted or proposed solutions. It is hard to imagine how EDs can effectively combat future disasters and crises, such as Covid-19, without first optimizing regular day-to-day operations.
Too many EDs are forced to function in a reactionary mode without a clear vision for both the patient and the health system.
Understanding the Core Value of Emergency Medicine
We believe it is paramount to the future of emergency medicine that emergency physicians recognize their core value to society and embrace their ability to provide more holistic care outside the emergency department, without compromising their ability to care for critically ill patients in the physical location of the emergency department.
Reflecting on our own experience, most applicants for emergency medicine residency training programs cite their desire to help people as their primary motivation. In our years serving on emergency medicine residency selection committees, we have seldom read essays focused on an applicant’s desire to do procedures or to be able to tell cool cocktail stories. Yet, we would posit that most emergency physicians are more likely to remember the first thoracotomy, chest tube, central line, or emergency delivery than any of the first 10 people they treated. The true core competency of an emergency physician is being available. It is true that emergency physicians perform critical care medicine and are experts at resuscitation; however, they also evaluate and treat ingrown nails, bronchitis, and sprains and strains. Even in the ED, the need filled most often is being available for everyone who needs care, most of whom don’t have a true medical emergency. As such, emergency physicians are the “availablists.” We accept all patients at any time and there is no prescreening. Emergency physicians are always available.
Prior to the Covid-19 pandemic, patients were utilizing acute care at a growing rate. Despite federal initiatives designed to improve linkage of patients to primary care providers, primary care visits were falling, while emergency department and urgent care visits were rising. Patients frequently prioritize cost and convenience over seeing their own primary care provider, especially for acute unscheduled care. There is clearly a premium on being open and available. Affordability adds more value. The prospect of waiting for a few days for an appointment can be a deal breaker for today’s health care consumer. Hence, these consumers take their ailments (even those that clearly are not true medical emergencies) to the emergency department.
It is time to think about emergency care, rather than emergency departments. No one goes to their cardiology department. They see their cardiologist. Emergency medicine needs to foster the value of emergency physicians, rather than just emergency departments. Patients need expertise, not a location. In some cases, they need (or think they need) immediate care in the emergency department. In other situations, emergency care can be safely provided in other locations, such as urgent care centers, retail clinics, ambulatory offices, or locations not traditionally thought of as medical — home, place of employment, or virtually anywhere. For emergency physicians to remain the availablists, we believe emergency physicians should lead the changes proposed here. The skill set does not change — just the location.
Moving Emergency Care Outside the Emergency Department
One framework for assessing emergency care in the emergency department is the input-throughput-output model.
Input must focus on the three main types of patients who come to the ED: emergency care, unscheduled but nonemergency care, and safety net care.
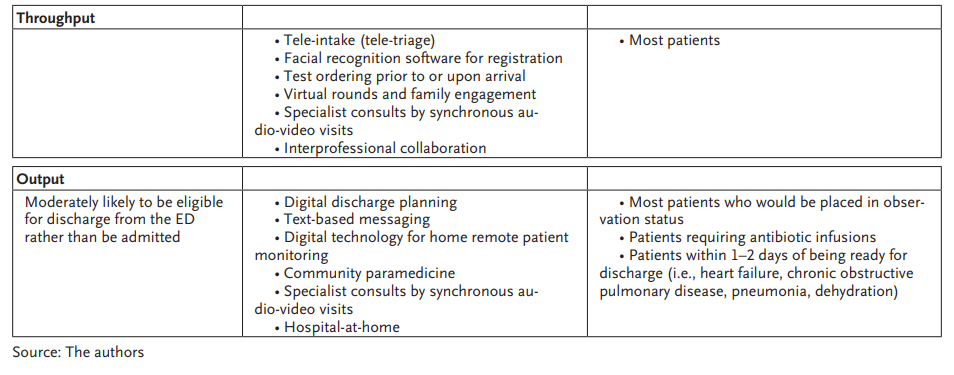
Throughput focuses on the internal processes within the ED: triage, registration, testing, and treatment.
Output focuses on moving patients into hospital beds or discharging them home with appropriate care linkages.
It is time to think about emergency care, rather than emergency departments.
It is time to think about emergency care, rather than emergency departments.
We believe the biggest impact on delivering emergency care outside the emergency department comes from a combination of strategies that affect all three components of the input-throughput-output model (see Table 1).

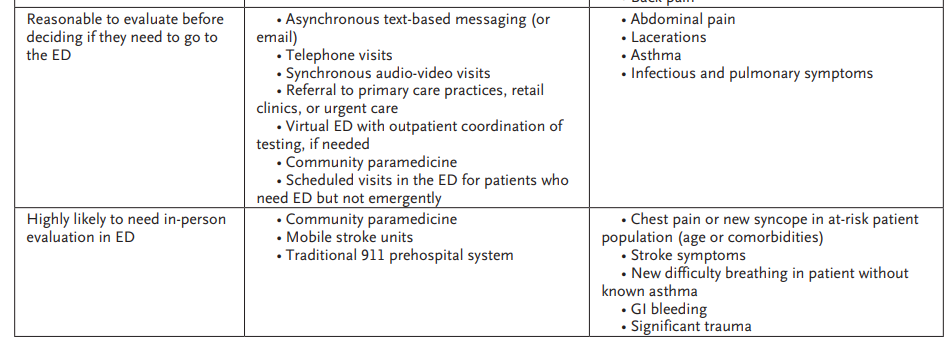
Input
Ideally, a change in input will facilitate initiating or providing care outside of the emergency department. Making nonemergent and safety-net care available through different channels is one strategy often discussed. This change will require a realignment of incentives (i.e., reimbursement and salaries) to encourage more primary and specialty providers to deliver care on evenings and weekends. This change also necessitates the elimination of obstacles encountered by primary care providers and specialists providing acute or subacute care. The requirement by payers for preauthorization leads to the paradigm of “the easiest way to get a test is to send the patient to the ED.” This approach must change to reduce input.
The growth of urgent care centers and retail clinics has not become a cost-effective substitute for emergency care, but rather has turned out to be a more convenient alternative to primary care. Although studies in the last decade have yielded conflicting results on this topic,-a recent study found that for each reduction in a low-acuity emergency department visit, there were 37 additional urgent care visits. Although the study did not address the necessity of care, it found that despite reduced higher expenses associated with ED visits in this study, the easy-to-access and convenient use of urgent care centers resulted in higher overall spending on low-acuity care.
The biggest impact on delivering emergency care outside the emergency department comes from a combination of strategies that affect all three components of the input-throughput-output model.
Telemedicine can be leveraged for acute and urgent care in lieu of emergency department visits with a high likelihood of minimizing emergency department and urgent care center referrals.,,,The most common type of emergency care telemedicine is a synchronous audio-video visit between a patient and provider. Although some health systems provide these services directly, many use a “provider network” such as Teladoc Health or MDLive. Asynchronous alternatives such as e-visits, chat-bots, or text message platforms can use artificial intelligence or live providers, and may be able to advise patients on where they can receive the indicated amount of care based upon their responses to a symptom-specific questionnaire.
We believe the future of emergency care will involve development of a “virtual ED” where emergency care providers can render remote care in a lower-cost environment. For some patients, this can be performed through a smartphone app, and they may not require further diagnostic testing. For other patients, it may require a telemedicine assessment with referral for expedited diagnostic testing (e.g., imaging, electrocardiography, and labs) in outpatient facilities, urgent care centers, or the hospital, with processes established so that patients can walk in and receive testing, then walk out and receive their follow-up recommendations virtually. For others, it may be a referral to the appropriate primary care physician or specialist, or a home visit by a community paramedic with or without telemedicine backup. The growing suite of services and advances in the virtual health care arena will give rise to some providers becoming virtualists.
At Jefferson and NYP-Weill Cornell, only 5–10% of our on-demand synchronous telemedicine calls get referred to the ED.
At Jefferson and NYP-Weill Cornell, only 5–10% of our on-demand synchronous telemedicine calls get referred to the ED.
Throughput
Once a patient arrives in the ED, strategies that expedite triage, testing, consulting, and treatment initiation can shorten the time the patient must spend in the ED.
The growth of urgent care centers and retail clinics has not become a cost-effective substitute for emergency care,but rather has turned out to be a more convenient alternative to primary care.
Virtual rounds (also known as family engagement) connect caregivers and family members with patients in real time while the patient is in the ED and may improve post-discharge coordination and communication.
We believe simply allowing family members to be present at the bedside, in person or remotely, can help improve understanding, speed ED throughput, and minimize challenges encountered at ED discharge. Telemonitoring, which reduces morbidity and mortality outside the ED, can assist themultiple other interventions aimed at reducing falls and improving quality of care in the ED.,
Interprofessional collaboration delivers expertise to a patient without face-to-face contact. With interprofessional collaboration, the consult is called. The consulting clinician reviews the medical record, discusses the case with the ordering clinician, and leaves a formal note in the chart. Interprofessional collaboration dramatically improves with response time (clinicians don’t need to travel) and allows the emergency physician to gain formal documented expertise of a specialist rather than the informal undocumented “drive-by” or “curbside” consult.
Output
ED boarding, or an inability to move admitted patients to an inpatient ward, is almost universal. Nothing has successfully solved this problem.
Community paramedicine programs typically target individuals who are at high risk of seeking recurrent care. Hospital-at-home programs target individuals who would otherwise be admitted but have social support networks and can receive what would otherwise be in-hospital care, delivered at home. These programs are complicated and require harmonization of multiple supply chains, such as pharmaceuticals (fluids, medications), digital monitoring technology, telemedicine capabilities, and in-home in-person care. Drone delivery will likely play a role here. As reimbursement for community paramedical and hospital-at-home programs grow, we expect to see improvements in emergency department throughput due to earlier discharge of patients who currently meet criteria for inpatient care.
The Emergency Department of the Future
As we stated earlier, EDs cannot be eliminated completely.
However, given the expected changes in emergency care delivery, and the consumerization of health care, the design and operational workflows must be reconsidered and optimized.-,
The emergency department will likely continue to serve as the physical entry point for many hospital admissions.
However, it will need to be redesigned. The concept of a large shared “waiting room” is no longer acceptable.
EDs will need to create other types of smaller “waiting rooms” or “holding areas” that eliminate risk of infectious transmission and maintain privacy.
Furthermore, improvements in methods to rapidly disinfect and turn over rooms will be a priority.
EDs cannot be eliminated completely …
… the design and operational workflows must be reconsidered and optimized (considering infection control as well)
The future of emergency care will involve development of a “virtual ED” where emergency care providers can render remote care in a lower-cost environment.
The future of emergency care will involve development of a “virtual ED” where emergency care providers can render remote care in a lower-cost environment.
Irrespective of the form and space, technology will be at the core of all future emergency departments.
Commencing upon arrival, every single aspect of the patient encounter will be infused with technology.
Imagine care beginning asynchronously via text, e-visit, or chatbot.
Then, if necessary, the care can be escalated to a synchronous audio-video visit.
- At Jefferson, 75% of acute care episodes are resolved at this point.
- In 2021, 80% of the remainder (20%) are referred to non-ED care locations, but we expect most of these referred cases will complete their care, either at their primary physician (possibly by leveraging apps to identify late cancellations and to secure those cancelled spots), or at home via community paramedicine (possibly using drone delivery of required equipment).
Irrespective of the form and space, technology will be at the core of all future emergency departments.
Of the approximately 5–10% of virtual-platform patients who currently require an in-person visit in the ED, many may be able avoid wait times by securing appointments and just arriving at their given time.
Apps may be able to eliminate the need for waiting rooms because they will be able calculate travel time, integrate with mass transit or traffic patterns, and even direct the patient to an available parking spot.
The same app can provide walking directions to the ED. Upon arrival, kiosks, facial recognition technology, or QR codes will facilitate efficient and contactless screening and registration.
Tele-triage programs can see patients even before arrival.
Laboratory tests and radiographic studies can be accomplished before patients are placed in a treatment room.
Patients requiring admission can complete most of the input processes before arrival, thereby markedly expediting throughput.
Discharge packages with easy-to-enable digital technology will become commonplace and increase the number of patients eligible for discharge with good outpatient follow-up, community paramedicine visits, or hospital-at-home, thus reducing the wait for hospital beds, thereby improving output.
Impact on Equity
Emergency departments serve an important safety-net role. Thus, moving care out of the emergency department is not without risk. It is also commonly believed that telemedicine can exacerbate disparities due to a lack of technological resources for people living in rural and urban underserved areas. There is a clear digital divide with gaps in telemedicine adoption based on education, income, and racial/ethnic background.,Technology access and digital literacy are essential to the effective use of telemedicine, and both are considerably lower among individuals with limited resources.-
But digital readiness includes more than just technology.
Other barriers include trust, acceptance, and relevance of telehealth as a means of receiving care.,,
For example, a survey of 162 African American patients with diabetes found that more than 90% of patients had sufficient access to the technology needed to engage in telehealth (device and Internet services), but only 39% had participated in a telehealth visit.
Lack of trust in physicians and living in more deprived neighborhoods were most strongly associated with failure to use telemedicine.
The emergency department will likely continue to serve as the physical entry point for many hospital admissions. However, it will need to be redesigned.
Despite the digital divide, there are opportunities for telemedicine to decrease care disparities.
Direct-to-consumer telemedicine allows access without an insurance requirement, unlike many office-based practices. Charges to patients are usually lower than those generated by office-based visits.
Telemedicine delivers remote expertise such as behavioral health and neuro-stroke care to rural emergency care settings where this expertise would otherwise not be available.
For now, we believe identifying those patients most in need of assistance to support telemedicine visits is a reasonable approach.
One novel idea, recently published, used an automated “video visit technical risk score” tool in the electronic health record to identify patients who would require technical assistance prior to their visits.
Using just presence or absence of an online patient portal, ability to do an eCheck-in process and presence or absence of a video visit in the preceding 3 months, they identified the 15% to 20% of patients who fell into the highest-risk categories.
Emergency care providers now have a unique opportunity due to the shift in patient priorities, payment reform, and Covid-19.
We have always been available in the emergency department.
Now, we should also be available where our patients want us, which is becoming increasingly likely to be in their backyards (urgent care or retail clinic) or on their phone (telehealth).
We should not define emergency care providers by their location in the literal “acute care space” any more than a cardiologist should be defined by their third-floor office.
We are always open, always available. We are the availablists.
We should not define emergency care providers by their location in the literal “acute care space” any more than a cardiologist should be defined by their third-floor office.
As emergency department volumes adjust, emergency care providers will likely find increasing opportunities to also be available in the pre-acute care phase when patients are just a “little sick”, and maybe finally take advantage of the opportunity to play a role in post-acute care.
Emergency care providers must develop a fluid skill set that can be leveraged outside of the emergency department, and the future strength of emergency departments will depend on the ability to devise and invest in comprehensive programs and technological platforms, which can easily shift or adapt in the face of a health crisis or disaster.
About the authors & affiliations
Judd E. Hollander
- Senior Vice President, Healthcare Delivery Innovation and Associate Dean, Strategic Health Initiatives, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, Pennsylvania, USA; Professor, Department of Emergency Medicine, Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, Pennsylvania, USA
Rahul Sharma
- Professor and Chairman, Department of Emergency Medicine, Weill Cornell Medicine, New York, New York, USA; Founder and Executive Director, Center for Virtual Care, Weill Cornell Medicine, New York, New York, USA; Emergency Physician-in-Chief, NewYork-Presbyterian/Weill Cornell Medical Center, New York, New York, USA
Originally published at https://catalyst.nejm.org on December 21, 2021.
Appendix: Table of Contents (TOC)
Introduction
Emergency Medicine Is at the Breaking Point
Understanding the Core Value of Emergency Medicine
Moving Emergency Care Outside the Emergency Department
- Input
- Thoughput
- Output
The Emergency Department of the Future
Impact on Equity







