



This is a republication of the article below, with the title above. The 2nd part of the post, has a republication of an excerpt of the statistic above.
The Number of Biological Parents with Alcohol Use Disorder Histories and Risk to Offspring through Age 30
Addiction Behaviour
Derek B. Kosty, a,bRichard F. Farmer, aJohn R. Seeley, a,bKathleen R. Merikangas, cDaniel N. Klein, dJeff M. Gau, a,bSusan C. Duncan, aand Peter M. Lewinsohna
2021 Mar 1
Chief Researcher and Editor of the Portal
Joaquim Cardoso MSc.
the health transformation
research institute and knowledge portal
October 30, 2022
ABSTRACT
Objective
- We investigated associations between the number of parents with histories of alcohol use disorder (AUD) and several offspring (proband) variables through age 30: occurrence of AUD and, separately, alcohol dependence; onset age of the initial AUD episode; time to recovery from the first AUD episode; number of distinct AUD episodes; and cumulative duration of AUD across episodes.
Methods
- Offspring data were collected during four assessment waves of a longitudinal epidemiological study of psychiatric disorders with a regionally representative sample.
- The reference sample included 730 offspring with diagnostic data from at least one parent.
- Offspring were assessed with semi-structured diagnostic interviews between mid-adolescence and young adulthood and parents were assessed when offspring were approximately 24 years of age.
Results
- As the number of parents with AUD increased, offspring risk for AUD and alcohol dependence also increased.
- Latent growth model results indicated that offspring AUD risk trajectories increase in severity as a function of the number of parents with AUD.
- This pattern of results was not observed for other AUD course-related features in offspring (i.e., number of distinct episodes; months required for recovery from initial episode; cumulative duration across episodes).
Conclusions
- The number of parents with a history of AUD is associated with overall offspring risk for AUD and alcohol dependence and elevated AUD risk trajectories through age 30.
- The number of parents with AUD may be a more relevant risk factor for onset-related characteristics of AUD in offspring than for its longitudinal course.
The number of parents with a history of AUD is associated with overall offspring risk for AUD and alcohol dependence and elevated AUD risk trajectories through age 30.
ORIGINAL PUBLICATION (excerpt)
1. Introduction
Within the United States, 7.5 million children younger than age 18, or 10.5% of youth within this age group, are estimated to live with at least one parent with an alcohol use disorder (AUD) [ 1].
In addition, parental drinking behavior is consistently and strongly associated with future drinking behavior in offspring [ 2], including alcohol abuse and dependence [ 3– 13].
The observation that parental history of alcohol misuse is an important risk factor for AUD in offspring has led investigators to hypothesize that offspring risk may be amplified when both parents have histories of problematic alcohol use or AUD.
In a prospectively assessed community-based sample, for example, the number of parents with AUD predicted the progression from occasional to regular alcohol use in offspring but was not associated with an increased risk for offspring AUD by age 17 [ 9]. In contrast, population-based research has indicated that offspring who lived with a parent during an AUD episode had a higher risk of developing a substance use disorder compared to non-exposed offspring, and that risk was greatest when offspring were directly exposed to two parents with AUD [ 14].
The limited literature on the number of parents with AUD has focused primarily on offspring risk for hazardous alcohol use in general and not on specific AUD course-related features demonstrated over time.
Related research, however, suggests that the number of parents with AUD may also be related to course-related features such as the timing, magnitude, and duration of AUD risk; AUD episode recurrence; recovery status; and the diagnosis of alcohol dependence versus abuse. In representative community-based samples, for example, AUD recurrence and AUD-related impairment in probands were associated with an increased risk for AUD among first-degree family members [ 15, 16]. Studies with non-representative samples have similarly suggested that longer AUD episode durations and AUD recurrence are associated with greater familial risk [ 17, 18]. Findings from treatment or clinic-based samples also indicate that alcohol dependence is a stronger predictor of AUD in family members than alcohol abuse [ 19, 20]. Nonetheless, the extent to which the severity and natural course of problematic alcohol use in offspring is associated with the number of parents with AUD remains unclear.
1.1. The Current Study
Despite the commonality of AUD histories among parents and the documented familial transmission of risk, few studies have examined associations between the number of parents with AUD histories and AUD risk and course-related features among offspring (probands).
Knowledge of the additional risk afforded by two versus one parent(s) with AUD histories may help inform theoretical models of AUD development, contribute to an understanding of risk-related mechanisms, and advance preventive efforts to reduce the intergenerational conveyance of hazardous alcohol use by identifying persons who are at greatest risk for AUD-related impairment [ 21].
Data used in this research come from the Oregon Adolescent Depression Project (OADP), a community-based and multi-generational longitudinal study in which psychiatric and substance use disorders in probands and first-degree relatives were assessed with structured interviews referenced to DSM criteria [ 22– 24].
Large-scale community-based studies on the parental transmission of AUD risk are uncommon, and those that do exist usually involve cross-sectional designs [ 7], judgments of parental AUDs based exclusively on offspring reports [ 7, 9], or non-standard assessments of alcohol abuse criteria [ 25]. Furthermore, family studies of AUD risk often involve clinical or high-risk samples that may lead to different conclusions concerning parental transmission of AUD risk, perhaps because of greater disorder severity found within these populations [ 26].
The present study overcomes these limitations and addresses four questions related to the parental transmission of AUD risk to offspring:
- Does overall risk for AUD in offspring through age 30 increase as a function of the number of parents with a lifetime history of AUD?
- What is the impact of the number of parents with AUD on offspring AUD risk trajectories through age 30?
- Do clinical features of AUD in offspring (i.e., cumulative duration across episodes, number of episodes, months required for recovery from initial episode, lifetime alcohol dependence versus abuse diagnosis) differ as a function of the number of parents with a lifetime history of AUD?
We hypothesized that as the number of parents with AUD increases, overall offspring risk for AUD will likewise increase.
We also expected corresponding increases in the intercept and slope of offspring AUD risk trajectories through age 30 and in the severity of AUD course-related features in offspring.
2. Methods
See the original publication
3. Results
See the original publication
4. Discussion
The purpose of this study was to examine associations between the number of parents with AUD and AUD-related outcomes in offspring.
We found that as the number of parents with AUD increased, offspring risk for AUD and alcohol dependence also increased.
Latent growth model results indicated that offspring AUD risk trajectories may increase in severity as a function of the number of parents with AUD.
The probability of meeting criteria for AUD during the initial age interval of 14 to 15.9 was approximately 2% if zero parents had an AUD history and 6% if one or two parents had an AUD history.
Offspring without parental histories of AUD and those with one parent with an AUD history experienced similar slopes in risk trajectories that peaked during the age interval of 20 to 21.9 years, with risk probabilities of 14% and 17%, respectively.
Although slopes did not statistically significantly differ across parent AUD groups in the conditional growth models, descriptive results suggested that offspring with two parents with AUD histories may have experienced a more sustained risk trajectory that peaked during the age interval of 24 to 25.9 years, with a risk probability of 25%.
Overall, findings are consistent with other research that suggests the number of parents with AUD predicts elevated risk for offspring alcohol use or AUD [ 9, 14].
We also examined whether course features associated with offspring AUD differed as a function of the number of parents with a lifetime history.
We found that offspring risk for alcohol dependence versus abuse increased 15% if one parent had a history of AUD and 20% if two parents had a history of AUD relative to offspring with no parental AUDs.
This finding is consistent with those of other studies in which alcohol dependence was associated with greater familial risk for AUD [ 19, 20]. Other course indicators of offspring AUD severity (i.e., cumulative duration of AUD, time required for recovery from initial AUD episode, and the number of distinct AUD episodes) were not significantly associated with the number of parents with a lifetime history of AUD.
Contrary to these findings, previous research suggests AUD recurrence and duration of episodes are associated with greater familial risk for AUD [ 16– 18].
Differences in results may be partly explained by methodological features.
This study utilized a top-down design emphasizing AUD risk among offspring in relation to parental AUD histories.
Previous research involved first-degree relatives in addition to parents [ 17, 18] and separate alcohol abuse and dependence diagnostic categories [ 16].
Analyses revealed that parental histories of AUD, as well as the number of parents with such histories, are associated with some AUD course features and severity indicators.
Findings generally indicated that any history of parental AUD was associated with greater risk for AUD and alcohol dependence through age 30 and a more severe risk trajectory.
Although the number of parents with AUD histories was associated with onset-related characteristics of AUD in offspring, it had little relevance in accounting for statistically significant variation in course-related features.
This study has several strengths …
… including the use of a large regionally representative community-based multigenerational sample, prospective evaluation of proband psychopathology, and semi-structured diagnostic interviews for diagnostic assessments of both parents and probands.
Study limitations included …
… sample characteristics and design features. Participants were relatively homogenous with respect to race and geographic location.
The generalizability of our findings to more diverse groups of individuals or locations is unclear. Parents were assessed at only one time point (~T 3), increasing the potential for retrospective recall bias in the measurement of parental AUD [ 44]. Potential mechanisms of the transmission of AUD risk from parents to offspring include both genetic [ 45] and environmental factors [ 46], but the current study was not designed to test the specific source of influence. Parents may or may not have met criteria for AUD while parenting, thus limiting inferences concerning effects of direct exposure (e.g., alcohol-specific behavior modeling). Only biological parents were included in this study, which ignores the possible role of step-parents with alcohol problems on proband AUD risk. Statistical power was limited for tests of differences in offspring AUD course-related features by parent AUD group, resulting in limited power to detect potential clinically meaningful differences in AUD course-related features between groups.
Descriptive results, for example, indicated that the cumulative duration of AUD was 10.9 months greater for offspring with two versus one parent with AUD; however, the difference in means was not statistically significant. These and other findings related to AUD course-related features in offspring should therefore be interpreted with caution.
Finally, the role of potential biases associated with proband attrition on study findings are unknown. Although discontinuation of study participation between waves T 1 and T 2 was greater for males and probands with a history of substance use disorder at T 1 [ 23], it was not greater for those with AUD specifically [ 36]. Discontinuation after T 3 was, however, more common among those with an AUD history by T 3 [ 36].
Because there were few other differences between study discontinuers and completers [ 28, 47], we are unable to draw informed conclusions about the degree to which attrition biased results.
4.1. Conclusion
Few studies have examined associations between the number of parents with AUD and AUD-related outcomes in offspring.
In this study, we found that the number of parents with a lifetime history of AUD is associated with overall offspring risk for AUD, elevated AUD risk trajectories through age 30, and greater risk for alcohol dependence.
These results may be translated into clinical settings where parental histories of AUD are used to identify candidates for targeted intervention and prevention programs.
Additional research based on more diverse samples is indicated, as are well-controlled tests of hypotheses concerning the mechanisms through which parental AUD increases offspring risk.
- Prospective evaluation of alcohol use disorder in a representative community sample
- Semi-structured interviews for diagnostic assessments of probands and parents
- Number of parents with AUD increased offspring risk for AUD and alcohol dependence
- Parent AUD histories predict increased severity of offspring AUD risk trajectories
- Offspring sex did not moderate associations between parental AUD and offspring risk
References
See original publication
About the authors & affiliations:
Derek B. Kosty ,a,b
Richard F. Farmer ,a
John R. Seeley ,a,b
Kathleen R. Merikangas ,c
Daniel N. Klein ,d
Jeff M. Gau ,a,b
Susan C. Duncan ,a and
Peter M. Lewinsohna
a Oregon Research Institute,
1776 Millrace Drive, Eugene, OR 97403, USA.
b University of Oregon,
College of Education, 1585 E 13th Ave, Eugene, OR 97403, USA.
c National Institute of Mental Health,
35A Convent Drive, MSC #3720, Bethesda, MD 20892, USA.
d Stony Brook University,
Psychology B Building, Stony Brook, NY 11794, USA.
Originally published at https://www.ncbi.nlm.nih.gov.
Keywords: Alcohol use disorders (AUD), parental AUD, number of parents, clinical features, trajectories
REFERENCE PUBLICATION (excerpt)

Introduction:
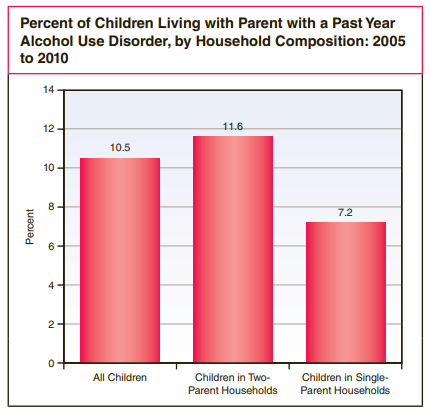
- An annual average of 7.5 million children younger than the age of 18 (10.5 percent of all children; Figure) live with a parent who had an alcohol use disorder in the past year.1
- These children are at a greater risk for depression, anxiety disorders, problems with cognitive and verbal skills, and parental abuse or neglect.2
- Furthermore, they are 4 times more likely than other children to develop alcohol problems themselves.3
Children may be exposed to family alcohol problems regardless of their household composition.
- According to the 2005 to 2010 National Surveys on Drug Use and Health (NSDUHs), of the 7.5 million children living with a parent with an alcohol use disorder,
- most of these children (6.1 million) lived with two parents and either one or both of these parents had an alcohol problem.
- However, 1.4 million children lived in households with single parents who had alcohol use disorders.
- In these households, 1.1 million children lived with a mother, and 0.3 million lived with a father.
There are many resources to help children when a parent has an alcohol problem (in the US)
The National Association for Children of Alcoholics (http://www.nacoa.org/) provides information and resources for professionals who work with these families. For additional resources, visit http://www.samhsa.gov/treatment/.
References
1 Alcohol use disorder includes dependence or abuse of alcohol and is based on definitions found in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). See American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th edition). Washington, DC: Author.
2 Substance Abuse and Mental Health Services Administration. (2004). Children of alcoholics: A guide to community action. Retrieved from http://store.samhsa.gov/shin/content/MS939/MS939.pdf
3 Anda, R. F., Whitfield, C. L., Felitti, V. J., Chapman, D., Edwards, V. J., Dube, S. R., & Williamson, D. F. (2002). Adverse childhood experiences, alcoholic parents, and later risk of alcoholism and depression. Psychiatric Services, 53(8), 1001–1009.