Health Systems Transformation (HST)
Research Institute and Knowledge Portal
Joaquim Cardoso MSc*
Chief Researcher, Editor and Strategy Officer
November 13, 2022
*MSc from London Business School — MIT Sloan Masters Program
Source: Eric Topol
ORIGINAL PUBLICATION (full version)
Clinical Whole Genome Sequencing
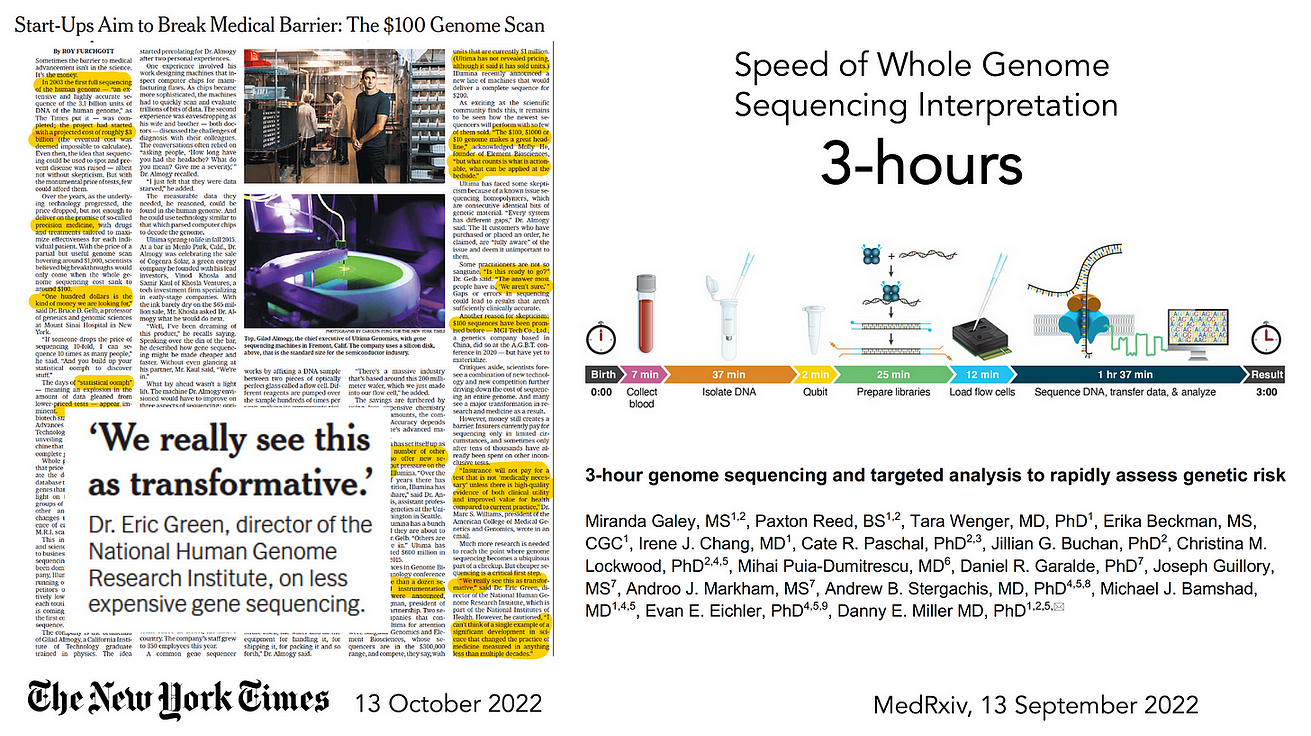
So much attention has been placed on the cost of whole genome sequencing (WGS) over the years, from about $300 million for the first one in 2000 ( some estimates are as high as $3 billion), to now starting to approach $100.
That’s a long sought and remarkable reduction in cost.
So much attention has been placed on the cost of whole genome sequencing (WGS) over the years, from about $300 million for the first one in 2000 ( some estimates are as high as $3 billion), to now starting to approach $100. That’s a long sought and remarkable reduction in cost
But what is equally impressive is that a team at the University of Washington, led by Danny Miller, set a world record in September 2022, reducing the time from sample (at birth of a baby) to interpretation to 3 hours!
But what is equally impressive is that a team at the University of Washington, led by Danny Miller, set a world record in September 2022, reducing the time from sample (at birth of a baby) to interpretation to 3 hours!
That diagnosis (of lacking the pathogenic gene variant of concern) in a newborn was facilitated by knowledge of familial risk.
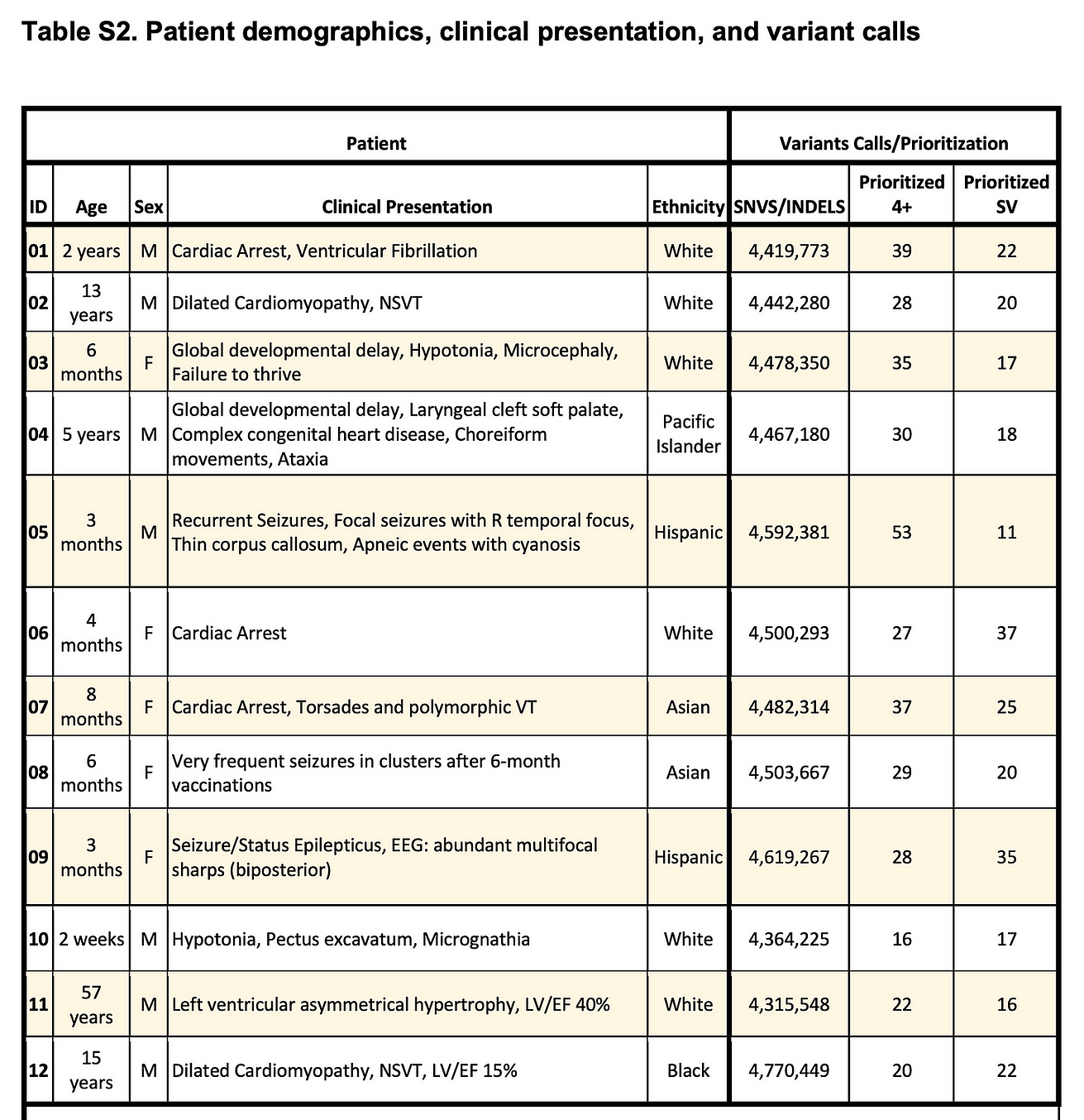
Nevertheless, that acceleration of sequencing and analysis comes in the wake of the Stanford team, led by Euan Ashley, performing WGS in 12 people ranging from 3 months to 57 years, in a critical care setting, in as little as 7 hours and 18 minutes.
Stanford team rapid sequencing of 12 patients in critical care setting with molecular diagnosis made in 5 individuals, Table below.
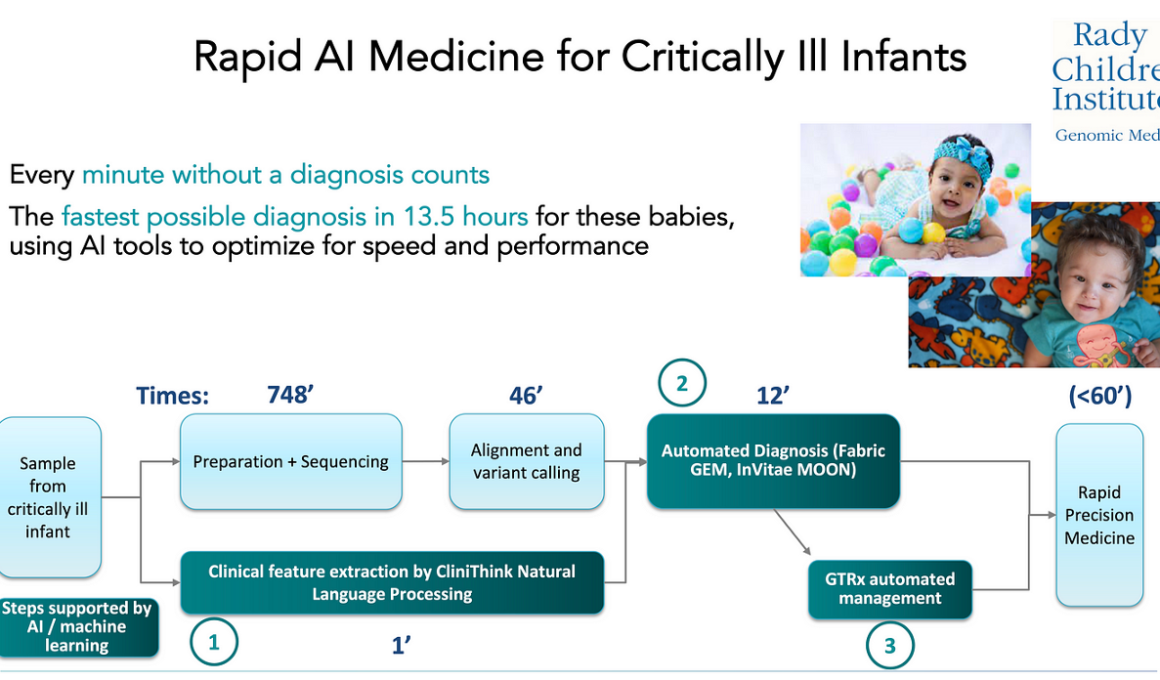
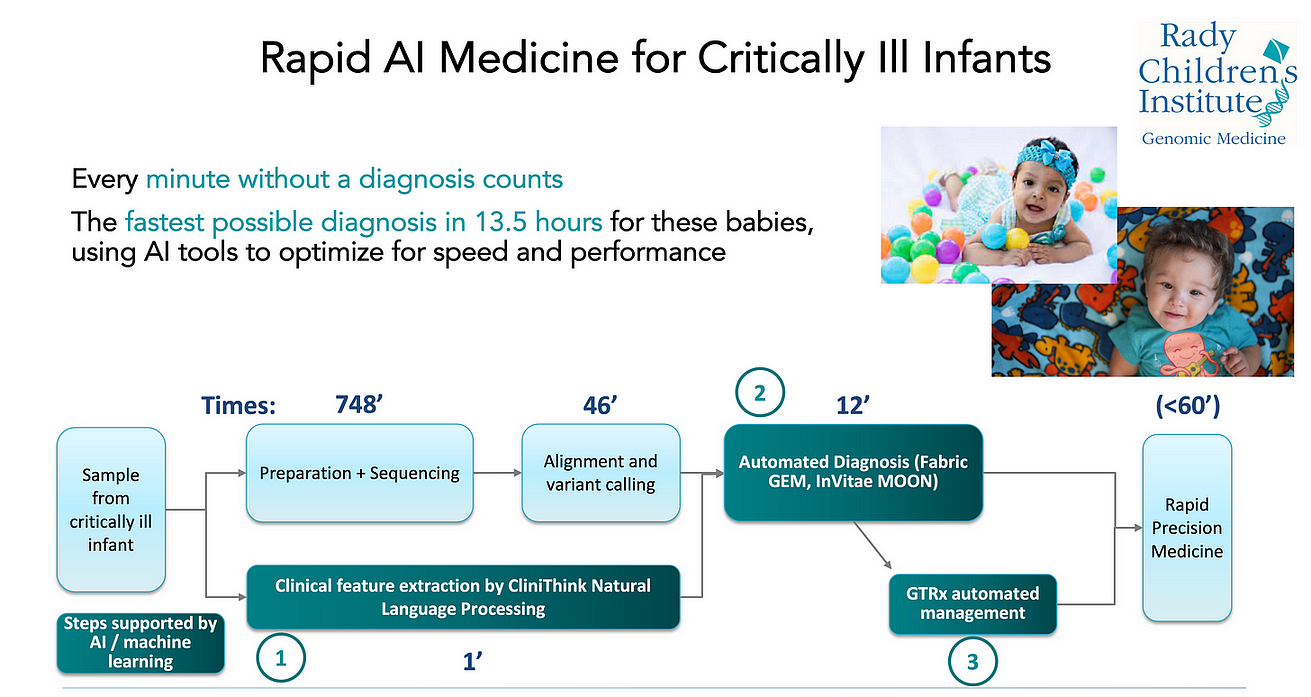
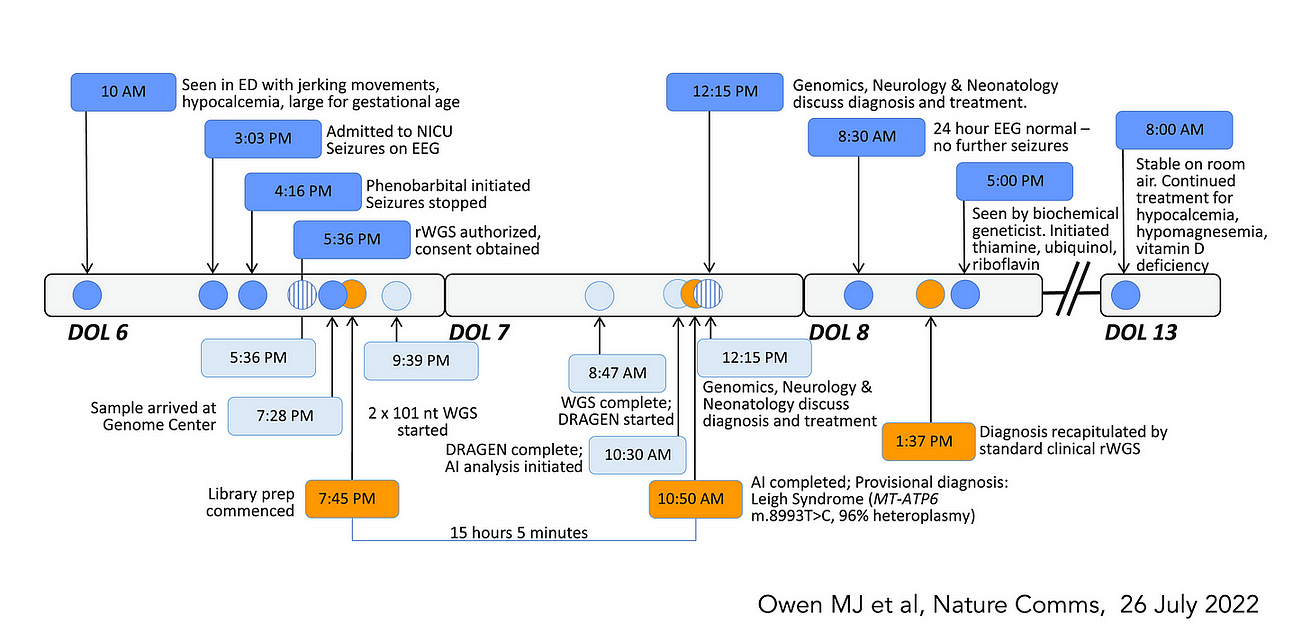
At Scripps Research, our SRTI team works closely with Rady Children’s Institute for Genomic Medicine, the group that has pioneered WGS in sick newborns who do not have a diagnosis, …
… accomplishing this from sample to interpretation and management recommendations all within 13 hours, using multiple AI tools (labelled 1–3 below) to expedite the readout and care of the baby.
At Scripps Research, our SRTI team works closely with Rady Children’s Institute for Genomic Medicine, the group that has pioneered WGS in sick newborns who do not have a diagnosis, …
… accomplishing this from sample to interpretation and management recommendations all within 13 hours, using multiple AI tools to expedite the readout and care of the baby.
Here is a recently published example of a baby with successful treatment that was readily initiated after the WGS diagnosis of Leigh Syndrome was made.
That success story is one of several hundred with this program in sick newborns now operational in 83 children hospitals in the United States and Canada.
Just think of the number of babies who have had irrevocable brain damage prevented or lives saved as a result of this initiative.
It’s unusual when there is a major innovation in medicine to start with neonates and children rather than adults. I actually can’t think of one offhand.
Certainly WGS use in acutely ill patients has not yet been applied to adults, although elective use of WGS for diagnosing rare and unknown conditions has been occuring more at select academic centers in recent years.
Now that WGS has gotten better (more complete and accurate), faster, and cheaper, will it become used more widely in adults?
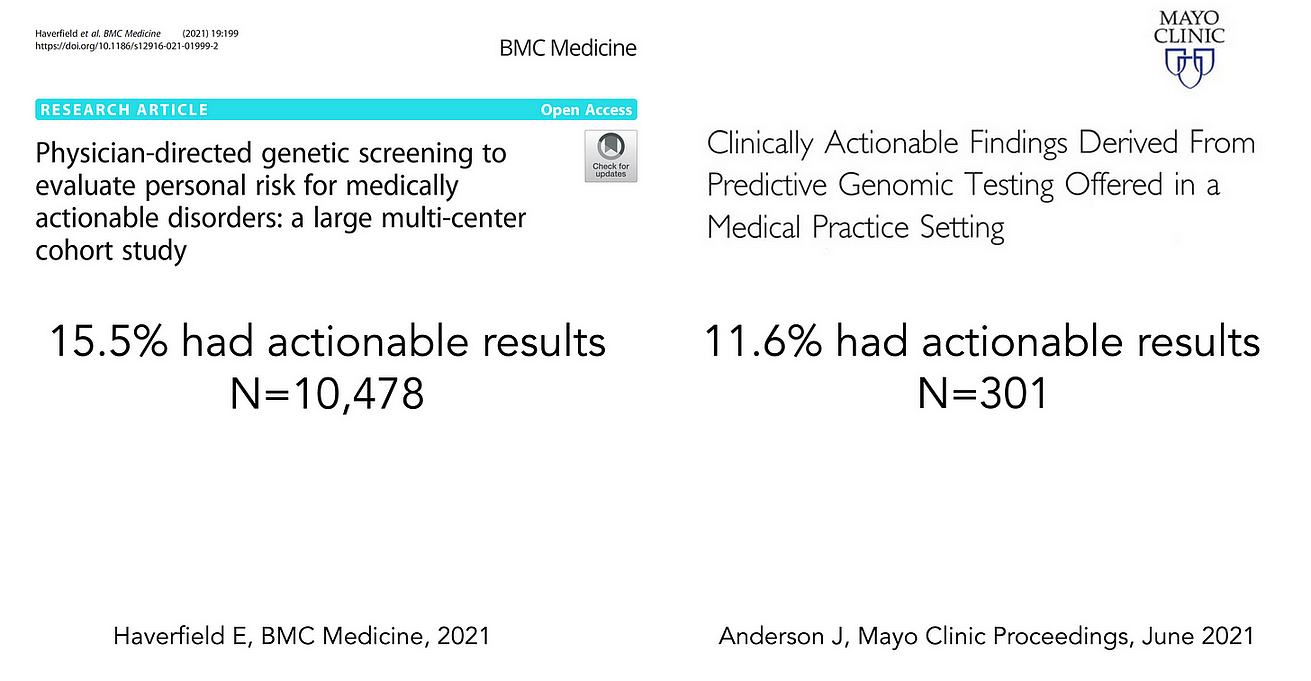
There are 2 fairly recent reports, here and here, that have shown that gene panels (sequencing just up to 147 genes) or WGS can be highly informative, picking up ~12–15% of healthy people with actionable results, such as important cancer or cardiovascular pathogenic mutations in individual without a family history, or Factor V Leiden, posing a significant risk of clotting.
The >10% level is noteworthy.
If we did a clinical trial with an intervention, such as a drug or device, and found that 1 in 10 patients derived important benefit, that level of absolute benefit would be declared as exceptionally important.
Most randomized trials that are considered positive come with far less proof of benefit.
The >10% level is noteworthy. Most randomized trials that are considered positive come with far less proof of benefit.
The largest clinical trial that I led, with over 41,000 patients, demonstrated a survival benefit for 1 of 100 patients.
Another frame of reference would be the Covid vaccine trials, which showed an absolute reduction of 6 per 100 (or 0.6 per 10) for preventing symptomatic infections out to 2 months
To also point out, the potential for WGS is far more than just picking up pathogenic mutations, such as a person’s gene-drug interactions, carrier state, and polygenic risk for most common medical conditions (heart disease, cancer, diabetes, etc).
No less, there is no use of WGS yet in the acute setting, as we’ve seen in newborns, to help make the diagnosis when it is elusive.
The reduction in cost and time for whole genome sequencing is historic and one of the most important advances that has occurred in life science in recent years.
With the increasing use of AI tools to make the variant calling and interpretation more accurate and rapid, …
… along with contextualizing the medical literature for a molecular diagnosis and possible treatment, …
… this could become someday an exemplar, beyond prediction of protein folding from amino acid sequence (AlphaFold), for AI’s contribution to biomedicine.
Hopefully some day we will harness its value to advance individualized medicine.
Originally published at https://erictopol.substack.com on November 13, 2022.
Names mentioned
University of Washington, led by Danny Miller, set a world record in September 2022,
Stanford team, led by Euan Ashley
Mallory J. Owen1,2, Sebastien Lefebvre 3, Christian Hansen1,2, Chris M. Kunard4, David P. Dimmock 1,2,5, Laurie D. Smith1 , Gunter Scharer1 , Rebecca Mardach2,6, Mary J. Willis1 , Annette Feigenbaum2,6, Anna-Kaisa Niemi2,6, Yan Ding1,2, Luca Van Der Kraan1,2, Katarzyna Ellsworth1,2, Lucia Guidugli1,2, Bryan R. Lajoie4, Timothy K. McPhail4, Shyamal S. Mehtalia4, Kevin K. Chau1,2, Yong H. Kwon1,2, Zhanyang Zhu 1,2, Sergey Batalov 1,2, Shimul Chowdhury1,2,5, Seema Rego 1,2, James Perry2,6, Mark Speziale2,6, Mark Nespeca2,6,7, Meredith S. Wright1,2,5, Martin G. Reese 8, Francisco M. De La Vega8, Joe Azure8, Erwin Frise 8, Charlene Son Rigby 8, Sandy White8, Charlotte A. Hobbs1,2,6, Sheldon Gilmer 2, Gail Knight2,6, Albert Oriol1,2, Jerica Lenberg1,2,5, Shareef A. Nahas1,2, Kate Perofsky1,2,6, Kyu Kim1,2,6, Jeanne Carroll1,2,6, Nicole G. Coufal1,2,6, Erica Sanford1 , Kristen Wigby1,2,6, Jacqueline Weir4, Vicki S. Thomson4, Louise Fraser 4, Seka S. Lazare 4, Yoon H. Shin4, Haiying Grunenwald4, Richard Lee4, David Jones 4, Duke Tran4, Andrew Gross4, Patrick Daigle4, Anne Case4, Marisa Lue4, James A. Richardson4, John Reynders 3, Thomas Defay 3, Kevin P. Hall 4, Narayanan Veeraraghavan1,2 & Stephen F. Kingsmore 1,2,5