Site editor:
Joaquim Cardoso MSc.
The Health Strategist — research, strategy and implementation
September 28, 2022
This is a republication of the paper below, with the title above.
Analysing the impact of modifiable risk factors on cardiovascular disease mortality in Brazil
PLOS One
Renato Simões Gaspar , Leandro F. M. Rezende, Francisco Rafael Martins Laurindo
June 22, 2022
ABSTRACT
Objectives
- We have examined the impact of changes in modifiable risk factors on CVD mortality in 26 Brazilian states from 2005 to 2017.
Methods
- Data were acquired from the Global Burden of Diseases study (GBD) and official sources of the Brazilian government, totalling 312 state-year observations.
- Population attributable fractions (PAFs) were calculated to determine the number of deaths attributed to changes in each risk factor.
- Fixed-effects multivariable linear regression models were performed, adjusting for income, income inequality, poverty and access to healthcare.
Results
- Between 2005 and 2017, CVD deaths reduced by 21.42%, accompanied by
– a decrease in smoking (-33%) and
– increases in hyperglycaemia (+9.5%),
– obesity (+31%) and
– dyslipidaemia (+5.2%).
- Reduction in smoking prevented or postponed almost 20,000 CVD deaths in this period, …
- … while increased hyperglycaemia exposure resulted in more than 6,000 CVD deaths.
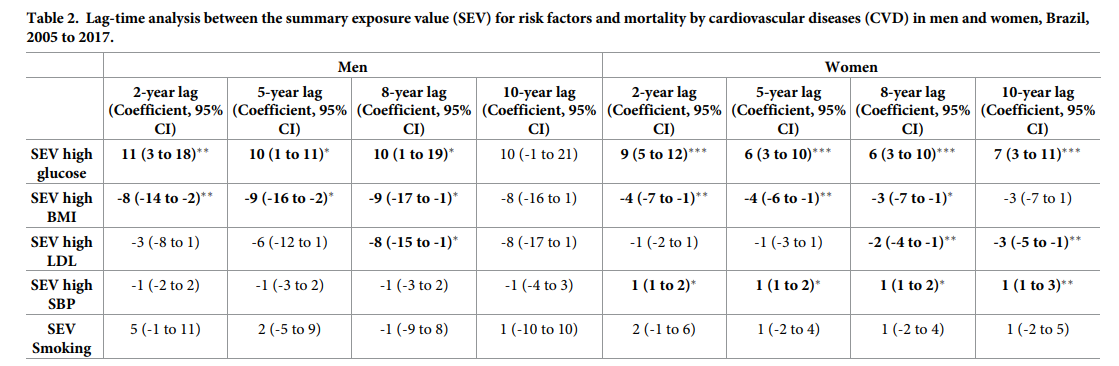
- The association between hyperglycaemia and CVD mortality was 5 to 10 times higher than those found for other risk factors, especially in women (11; 95%CI 7 to 14, deaths per 1-point increase in hyperglycaemia exposure).
- Importantly, the association between hyperglycaemia and CVD mortality was independent of socioeconomic status and access to healthcare, while associations for other risk factors after the same adjustments.
Reduction in smoking prevented or postponed almost 20,000 CVD deaths in this period, …
… while increased hyperglycaemia exposure resulted in more than 6,000 CVD deaths.
Conclusion
- Reduction in smoking was the risk factor that led to the highest number of CVD deaths prevented or postponed, …
- … while hyperglycaemia showed the most deleterious association with CVD mortality.
- Health policies should aim to directly reduce the prevalence of hyperglycaemia to mitigate the population burden of CVD in Brazil in the future.
Reduction in smoking was the risk factor that led to the highest number of CVD deaths prevented or postponed, …
… while hyperglycaemia showed the most deleterious association with CVD mortality.
Health policies should aim to directly reduce the prevalence of hyperglycaemia to mitigate the population burden of CVD in Brazil in the future.
Suggestions [excerpted from the paper]
These findings raise the need for an urgent debate on more effective policies to decrease hyperglycaemia and diabetes, such as:
- improvements in school nutrition,
- price policies to reduce the consumption of sugar-sweetened beverages and ultraprocessed food and
- curbing marketing and availability of these products (all of which were reviewed recently in [27, 28]).

Introduction
Cardiovascular diseases (CVD) are the leading cause of death in most low- and middle-income countries (LMICs), such as Brazil [1], despite a decreasing trend in mortality over recent years [2].
Among different types of CVD, ischaemic events, such as ischaemic stroke and ischaemic heart disease have the highest impact on the Brazilian population’s health [1].
Among different types of CVD, ischaemic events, such as ischaemic stroke and ischaemic heart disease have the highest impact on the Brazilian population’s health
The likelihood of developing CVD or dying from an ischaemic cardiovascular event is dramatically increased by the presence of common behavioural and metabolic risk factors, such as hyperglycaemia, obesity, dyslipidaemia, hypertension and smoking [3].
The likelihood of developing CVD or dying from an ischaemic cardiovascular event is dramatically increased by the presence of common behavioural and metabolic risk factors, such as hyperglycaemia, obesity, dyslipidaemia, hypertension and smoking
Among these, a recent prospective study has shown that diabetes and hypertension were the risk factors that led to the highest number of deaths due to cardiovascular events in low-income countries (LICs) [3].
However, it is unclear how different risk factors are associated with CVD mortality in LMICs, especially in countries with a universal healthcare system, given that primary care has been shown to decrease the population burden of CVD [4].
… a recent prospective study has shown that diabetes and hypertension were the risk factors that led to the highest number of deaths due to cardiovascular events in low-income countries (LICs) [3].
However, it is unclear how different risk factors are associated with CVD mortality in LMICs, …
In addition to metabolic and behavioural risk factors, it has been acknowledged that the burden of CVD differs between men and women.
On one hand, men display a higher mortality burden of CVD when compared to premenopausal women [5]. This trend is mostly equalized among elderly men and postmenopausal women [5].
In parallel, it was shown that women are more likely than men to present several concomitant risk factors (e.g. diabetic women tended to live more with obesity and dyslipidaemia than their male counterparts [6]). Despite this, women were less likely to be adequately treated for these conditions [6].
Altogether, it has been recognized that there are sex disparities with regard to the prevalence of risk factors and CVD mortality, however it remains yet unclear to what extent the trend of common risk factors is associated with the decrease in CVD mortality in LMICs, such as Brazil.
Importantly, there may be some sort of hierarchy among risk factors in which some are more relevant than others to explain the trend in CVD at the population level.
Therefore, we have investigated the association between several common behavioural and metabolic risk factors (hyperglycaemia, obesity, dyslipidaemia, obesity and smoking) and CVD using state-level information from 2005 to 2017 in Brazil.
In addition, we quantified how much of the decrease in CVD mortality between 2005 and 2017 could be explained by changes in the state-level prevalences of such risk factors.
Overall, our findings may help policymakers to implement more effective strategies to target these risk factors and therefore reduce the burden of CVD in Brazil.
Overall, our findings may help policymakers to implement more effective strategies to target these risk factors and therefore reduce the burden of CVD in Brazil.
Other sections
See the original publication

Discussion
This study provides a thorough analysis of the impact of modifiable risk factors on the decreasing trend for CVD mortality in Brazil.
Reductions in smoking led to the highest number of deaths prevented or postponed, while hyperglycaemia was the only risk factor with an impactful and robust association with CVD mortality, particularly for women.
The association between hyperglycaemia and CVD mortality was stable after comprehensive robustness checks and was independent of socioeconomic variables and access to healthcare.
Altogether, data herein gathered suggest that hyperglycaemia is associated with CVD mortality in the Brazilian
Overall, the age-standardized CVD mortality has been decreasing in Brazil over the last decades.
This could be due to socioeconomic factors, such as improved GDP per capita, educational levels and primary healthcare coverage, all of which were shown to be associated with decreased CVD mortality [3, 4, 17].
Moreover, we calculate that the marked reduction of smoking in the Brazilian population has prevented or postponed around 17000 deaths in both sexes combined.
Despite the annual reduction in CVD deaths observed thus far, it is likely that, as Brazil transitions to a high-income society, this trend may slow down or even reverse, as observed for several high-income countries [18].
In light of the need to find more effective strategies to reduce CVD mortality, we have explored the associations of the population exposure to common metabolic and behavioural risk factors with CVD events.
After comprehensive robustness checks it was evident that hyperglycaemia was the risk factor with the most robust and stable association with CVD mortality. In parallel, hypertension, but not hyperglycaemia, was associated with the incidence of CVD.
This is in agreement with a recent cohort study that showed that the magnitude of the association of diabetes and hypertension with CVD mortality was greater than that found for other metabolic risk factors in LICs [3].
However, we have not found stable associations between hypertension and CVD mortality in the Brazilian population.
It is possible that, due to a universal healthcare system and a significant increase in primary healthcare coverage, hypertension has had a lower effect on CVD mortality compared to LMICs without a universal healthcare system.
Indeed, effective universal healthcare can significantly reduce deaths due to CVD [19], while a global study showed that Brazil has a high proportion of control rate for hypertension when compared to other Latin American countries and LMICs [20].
Effective hypertension control has been shown to drastically reduce the risk of developing cardiovascular events [21].
In contrast, it is still unclear if the management of diabetes with glucose-lowering drugs can reduce CVD deaths, as exemplified by studies of widely-used metformin [22] and the new drug dapagliflozin [23].
We have found some sex disparities in how hyperglycaemia is associated with CVD mortality.
For instance, hyperglycaemia and diabetes were consistently associated with ischaemic stroke mortality in women but not in men.
This is consistent with previous studies showing that diabetes/hyperglycaemia is a stronger risk factor for stroke in women than it is in men [24, 25].
These sex-specific differences may be due to social, psychological or biological phenomena, although underlying social determinants of sex disparities are largely understudied [26].
Biologically it has been shown that women tend to have higher rates of obesity, hypertension and dyslipidemia and are less likely to receive adequate treatment for these conditions [6].
Altogether, our data agree with previous observations that hyperglycaemia/diabetes is more strongly associated with CVD mortality in women than it is in men (this topic has been summarized by an American Heart Association statement [26]) while we found no association with the incidence of CVD.
Our study has some implications for health policy.
First, data suggest that health policies should aim to directly reduce the prevalence of and exposure to hyperglycaemia in Brazil.
Second, the cushion provided by universal healthcare and improvements in primary care may not suffice to mitigate the deleterious effects of hyperglycaemia on CVD mortality.
These assumptions are corroborated by the high-magnitude association between hyperglycaemia and CVD mortality, which was stable even after adjusting for access to healthcare.
Therefore, the increase in the prevalence of diabetes might eventually be followed by increases in CVD mortality if different strategies are not implemented.
These findings raise the need for an urgent debate on more effective policies to decrease hyperglycaemia and diabetes, such as:
- improvements in school nutrition,
- price policies to reduce the consumption of sugar-sweetened beverages and ultraprocessed food and
- curbing marketing and availability of these products (all of which were reviewed recently in [27, 28]).
These findings raise the need for an urgent debate on more effective policies to decrease hyperglycaemia and diabetes, such as:
… improvements in school nutrition, price policies to reduce the consumption of sugar-sweetened beverages and ultraprocessed food and curbing marketing and availability of these products
However, the debate on the need for such policies and the evidence of their impact is still insipient, especially in developing countries such as Brazil.
However, the debate on the need for such policies and the evidence of their impact is still insipient, especially in developing countries such as Brazil.
We acknowledge several limitations in our study.
We have used estimates of risk factor exposure, which are based on observational studies by independent researchers and national surveys conducted by governmental entities.
It is therefore possible that the exposure to risk factors included individuals with a pre-existing cardiovascular condition, which could potentially influence our findings.
Despite the measurement error of exposures and outcomes that needs to be accounted for, data collected from IHME and the GBD study are the largest database of their kind and were consistent with a large prospective study linking modifiable risk factors and CVD mortality in 21 countries [3].
Mortality measurements might have been under-represented in Brazil, especially in poorer states [1].
However, the data used were still considered of high quality [1].
Data from IHME were smoothed by IHME [1], which could potentially mask subtle changes over time.
To overcome such limitations, fixed effects for state and time were used to reduce the likelihood of unobserved changes in mortality reporting being associated with changes in income inequality [29].
Data were aggregated to states, therefore further studies are needed to test associations observed in this study at the individual level.
Moreover, we are unable to make causal interpretations of models fitted, despite the use of fixed effects and relevant control variables.
Our results are supportive of a strong and stable association between hyperglycaemia and CVD mortality in Brazil, which seems to be more robust in women than in men.
The association between hyperglycaemia and CVD mortality may last for up to 10 years and may be independent of access to healthcare.
Indeed, changes in the population exposure to hyperglycaemia led to the highest number of deaths between 2005 and 2017 in both men and women, while the reduction in smoking led to the highest number of deaths prevented or postponed.
Sex disparities reiterate that diabetes and hyperglycaemia are stronger risk factors for CVD in women than in men.
Altogether, our findings provide evidence that strategies to reduce smoking were key to the reduction of CVD mortality observed in Brazil over the past decades, while there is an urgent need for policies that aim to decrease hyperglycaemia in the Brazilian population in order to mitigate the burden of CVD mortality.
… our findings provide evidence that strategies to reduce smoking were key to the reduction of CVD mortality observed in Brazil over the past decades, while there is an urgent need for policies that aim to decrease hyperglycaemia in the Brazilian population in order to mitigate the burden of CVD mortality.
References and additional information:
See the original publication
About the authors & affiliations:
Renato Simões Gaspar ID1*,
Leandro F. M. Rezende ID2 ,
Francisco Rafael Martins Laurindo 1
1 Laboratory of Vascular Biology,
Health Institute (InCor),
University of Sao Paulo School of Medicine, Sao Paulo, Brazil,
2 Departamento de Medicina Preventiva,
Escola Paulista de Medicina,
Universidade Federal de São Paulo, Sao Paulo, Brazil
Related publication:

Diabetes é a variável que mais impacta número de mortes por infarto
28 de setembro de 2022
https://agencia.fapesp.br/diabetes-e-a-variavel-que-mais-impacta-numero-de-mortes-por-infarto/39684/