That includes Data, AI, Digital, and Wearables and Smartphones, among others.
This is a republication of the article below, with the title above, with a focus on the topic in question, edited by Joaquim Cardoso MSc.
In ten years, AI leading and doctors supporting: reality or madness? — A Challenging View of AI Future
Interview with Prof. Dr. Folkert Asselbergs, cardiologist and Professor Precision Medicine in Cardiovascular Disease at UMC Utrecht and University College London
Ortec Magazine
Folkert Asselbergs, UMCU (University College, London)
№2 -2022
Folkert Asselbergs is a cardiologist at UMC Utrecht and is involved in several data collection and data analysis projects in the field of personalized medicine.
In the near future, Artificial Intelligence (AI) will play a much bigger role in healthcare, including in hospitals.
Asselbergs says: “At the moment, AI still plays a supporting role, but I think that ten years from now, AI will be in the lead and doctors will primarily support.”
“At the moment, AI still plays a supporting role, but I think that ten years from now, AI will be in the lead and doctors will primarily support.”
The past 18 months showed that healthcare planning is essential, especially in times of crisis. But data are not always readily available. Has the General Data Protection Regulation inhibited progress in data exchange?
Covid is the prime example of why healthcare needs to modernize, but red tape has started slowing development to the speed of molasses.”
Folkert Asselbergs does not hide his impatience.
AI is not widely used in healthcare yet, as many people do not yet see its added value.
Part of the reason is that the Netherlands is very restrictive in using and sharing data for research.
Making data available for research will be a game changer: it will allow for faster development of new and better algorithms and will boost innovation.
AI is not widely used in healthcare yet, as many people do not yet see its added value.
Part of the reason is that the Netherlands is very restrictive in using and sharing data for research.
Making data available for research will be a game changer …
Plenty of ideas are out there, the technology is ready, but the progress is not as fast as I would like to see it.
I would like to urge the Minister of Health to amend legislation and regulations more quickly: now is the time for action. The government has to facilitate data exchange before the next pandemic presents itself.”
I would like to urge the Minister of Health to amend legislation and regulations more quickly: now is the time for action. The government has to facilitate data exchange before the next pandemic presents itself.
Asselbergs often finds himself debating colleagues who are less convinced of the value of AI.
“For single sources of data, such as ultrasounds, MRIs and CT scans, AI is already advanced, and developments are forging ahead at blistering pace.
Integrating different data sources — particularly the unstructured text found in electronic health records — will take longer.
AI now still plays a supporting role, but I sincerely think that ten years from now, AI will be in the lead and doctors will primarily support.
AI now still plays a supporting role, but I think that ten years from now, AI will be in the lead and doctors will primarily support
We will still be the ones to talk to patients and make decisions about the suggestions put forward by AI, but I envision people coming into a car wash of sorts with imaging, biomarkers and wearable data, giving them a top five of the most likely diagnoses.
These are then mapped to existing scientific knowledge about what the therapy of choice should be for these types of patients. It would almost turn doctors into consultants.”
We will still be the ones to talk to patients and make decisions about the suggestions put forward by AI, …
… but I envision people coming into a car wash of sorts with imaging, biomarkers and wearable data, giving them a top five of the most likely diagnoses.
IN TEN YEARS’ TIME, AI WILL BE IN THE LEAD AND DOCTORS WILL SUPPORT. WHAT DO YOU THINK: REALITY OR MADNESS?
Source: ORTEC’s LinkedIn poll — 2021
CAPILLARIES OF SOCIETY
Will patients accept this change? Or will they be wary of having an algorithm determine what is best for their health?
“Discussions often revolve around ‘the human touch’, but who is to say that AI isn’t better at that, too?
You can take my word for it, there are some boorish doctors out there, and all the complaints we get revolve around communication.
You could really wonder whether people are truly more empathic than computers.”
The skeptical attitude to using AI adopted by many patients and colleagues can also be traced back to trust, or a lack thereof, in data, Asselbergs notes.
“The feeling of: is it correct? A particularly telling example was a study that used deep learning on chest x-rays in the emergency ward.
When they finally looked at the decisive feature of the prediction model, it turned out that the device used to take the images was the best predictor, because the Siemens device was used for bedridden patients and the Philips device for people who could still walk around.
These are important pitfalls to consider, hence the call for explainable AI: you want to know what’s under the hood.
These are important pitfalls to consider, hence the call for explainable AI: you want to know what’s under the hood.
Data from people in underprivileged social groups are rarely captured by algorithms, even though they’re the groups the algorithms are used for most.
That will be the most difficult challenge: getting to the capillaries of society.
We are now considering the idea of a form of donor registration for data.
If we don’t change the data inclusion, inclusiveness will be unachievable.
We are now considering the idea of a form of donor registration for data.
If we don’t change the data inclusion, inclusiveness will be unachievable.
Once the trust is there, we might be off to the races, especially when it comes to personal medicine:
I think that patients will soon have their own Amazon or Microsoft or ORTEC platform that automatically retrieves all your information, if you give it permission, which you could then enrich yourself by adding DNA, biomarkers or a scan.
The skeptical attitude to using AI adopted by many patients and colleagues can also be traced back to trust, or a lack thereof, in data.
That’s where algorithms are headed, but where are the risks?
You share your results with a doctor to ask them their opinion, and even this doctor will, likely, have been chosen by AI.”
With all these new technological possibilities, Asselbergs does foresee problems with regard to the different groups in society:
“Data from people in underprivileged social groups are rarely captured by algorithms, even though they’re the groups the algorithms are used for most.
That will be the most difficult challenge: getting to the capillaries of society.
We are now considering the idea of a form of donor registration for data. If we don’t change the data inclusion, inclusiveness will be unachievable
What developments can we expect in the shorter term? And to what extent does the Medical Device Regulation still raise practical issues for these types of AI applications?
The big med-tech behemoths are coming and will focus mainly on prevention.
They will steer clear from the curative side of things at first, because it is considerably more complex, due in part to the Medical Device Regulation.
Besides, there is simply not as much money to be made there. We will all have to discover how developments in hospitals unfold together.
The platform economy is already upon us: whoever has the platforms with the biggest user base, wins.
You don’t necessarily need to have the better product: scale is what matters. It’s a shame, to be honest, because it does slow down innovation.”
I think that patients will soon have their own Amazon or Microsoft or ORTEC platform that automatically retrieves all your information, if you give it permission, which you could then enrich yourself by adding DNA, biomarkers or a scan.
The platform economy is already upon us: whoever has the platforms with the biggest user base, wins.
You don’t necessarily need to have the better product: scale is what matters. It’s a shame, to be honest, because it does slow down innovation.”
THE WHOLE PATIENT
University College London, where Asselbergs is a part-time professor of Precision Medicine, employs data managers for each of its divisions.
Data scientists are mostly involved in the research side of healthcare, but Asselbergs can hardly imagine not having a data scientist in his department in ten years’ time:
“Someone who, when we discuss patients during the morning handover, can chart the optimal course based on the data. Data scientists are far from having the final say, but AI support will come to play an increasingly important role in healthcare decisionmaking.”
He believes the most important thing AI will bring to healthcare is patient empowerment, thanks to the democratization of data.
“The experience and knowledge gap between patients and doctors is enormous, including data knowledge. We speak our jargon and wear a white coat, all of which creates distance.
That distance will soon disappear because patients will know exactly what I know.
The USA is miles ahead of the Netherlands in terms of general knowledge of anatomy and which doctor to see.
In the Netherlands, people tend to think: you have a degree, you decide.”
If there’s one sector that can benefit from the increasing availability of more data and better AI, it’s healthcare.
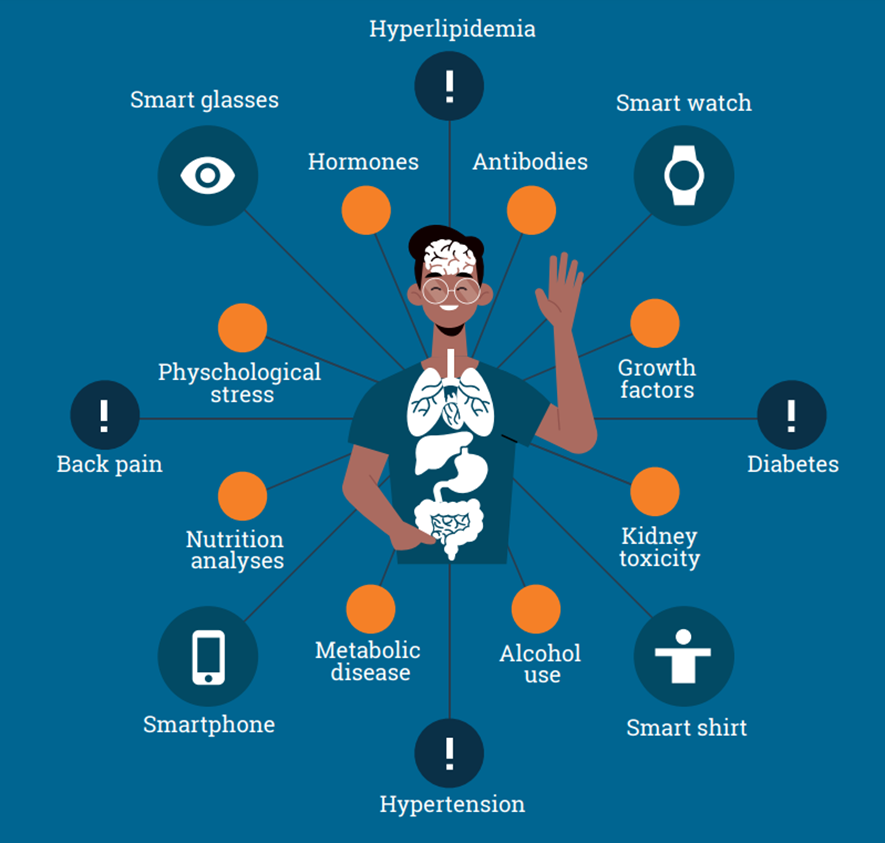
Wearables and smartphones generate more and more medical data than can be used for preventative measures and treatment plans.
Databases containing information on large numbers of patients can be used for personalized medicine.
That changes the role and business model of healthcare providers. Instead of treating existing medical issues, they will increasingly use data and AI to prevent problems, or treat them in earlier stages.
That changes the role and business model of healthcare providers. Instead of treating existing medical issues, they will increasingly use data and AI to prevent problems, or treat them in earlier stages.
Have medical schools incorporated these new insights about AI in their programs?
“Most have not. That’s why the DataClinics program is working on a Data Science basics curriculum for healthcare professionals. We need to prepare healthcare professionals for the future.
Specialisms are still very traditional and organ-centered, but that will change, and the question is whether specialisms as we know them will be around for much longer.
Specialisms are still very traditional and organ-centered, but that will change, and the question is whether specialisms as we know them will be around for much longer.
I think technical medicine is the profession of the future: it’ll prove to be essential.
Doctors will still need to do their rounds and listen to patients, but they will have to become communication experts or consultants, reasoning more from the perspective of the human being they are treating rather than their organs.
You could consider incorporating an internist into the surgery department, for instance, to help optimally treat patients with multimorbidity.
At the same time, that internist will be able to harness U-Prevent to tackle prevention issues, so that the GPs no longer have to.
Now that the patient is in hospital anyway, why not give them a quick check-up and treat their high blood pressure while they’re here?
Hospitals can still be very siloed at times.
With our new strategy, we get to see a much clearer picture of patients even before they come in for surgery.
We treat the whole patient: while you’re here to get a new hip, we’ll treat your cholesterol at the same time. It’s an approach that makes a lot more sense.
Originally published at https://ortec.com
Names mentioned:
Interview with Prof. Dr. Folkert Asselbergs, cardiologist and Professor Precision Medicine in Cardiovascular Disease at UMC Utrecht and University College London

Folkert Asselbergs
Professor Folkert W. Asselbergs has been working at UMC Utrecht as a cardiologist since 2010. He specializes in diagnosing hereditary cardiomyopathy and heart failure. Since 2013, he has also held a parttime position at the Institute of Cardiovascular Science and Institute of Health Informatics, University College London as Professor of Precision Medicine. Asselbergs has been head of Circulatory health at UMC Utrecht for two years and chair of the Data Infrastructure pillar of the Dutch CardioVascular Alliance.
In addition, he researches how genetic information and other data can be (re)used to individualize diagnostics, risk prediction and treatment of cardiovascular diseases.