Looking across world-leading organizations, we have identified six priority levers that health systems can apply in order to transition to a fundamentally different paradigm of outpatient care delivery, for all types of outpatient encounters.
BCG — Boston Consulting Group
By Ben Horner, John Gooch, and Ania Labno
19 MAY 2020
The COVID-19 crisis has triggered a revolution in how health systems deliver outpatient care. In a matter of weeks, ways of working that dated back to the mid-20th century, if not earlier, have been supplanted by a more patient-centric approach enabled by digital innovation. As the acute phase of the crisis subsides in many countries, health systems should seek to embed the positive changes.
Ambitions should extend far beyond sustaining incremental improvements. Indeed, health systems should pursue a full-scale paradigm shift for outpatient care. To design and implement the new paradigm, they should apply a set of levers across the three dimensions of outpatient encounters: initial diagnosis, episodic care (including elective surgery), and chronic disease management.
Health systems need to act quickly in order to build on the recent unprecedented momentum for change. To initiate a transformation, they must lock in the positive changes already made, gain clinicians’ support, set priorities, and secure funding. Once they identify successful innovations, they should accelerate deployment at scale through redesigned ways of working and effective governance.
Transforming at “COVID Speed”
In recent months, health systems have launched new care pathways at an unprecedented pace, moving at what some have dubbed “COVID speed.” For example, in the US, Providence St. Joseph Health rolled out automated care and remote-monitoring tools for COVID-19 patients in just four days, and in England, primary care practitioners transitioned from having 90% of consultations in person to providing 85% remotely in a matter of weeks.
It is imperative for outpatient departments (OPDs) to achieve this scope and pace of change as well. In fact, a paradigm shift in outpatient services is long overdue. In the original model of care, with roots in the 18th century, outpatients visited specialist physicians in their consulting rooms. Specialists had few diagnostic tools and seldom communicated with one another. In the 20th century, the outpatient model was revolutionized by the centralization of specialty care and diagnostic facilities in hospitals-and this model has largely persisted to the current day with only incremental changes.
Updating the antiquated model will be essential to help OPDs cope with levels of demand that had been rising for many years before the crisis. In the US, while inpatient stays steadily declined from 2005 through 2015, outpatient visits rose by 14%. In an even more dramatic upsurge, outpatient visits in the UK have doubled in the past decade to 94 million per year. A paradigm shift is also vital to help OPDs quickly clear the buildup of patients whose care has been postponed because of the pandemic. This backlog can be very large-typically 10% to 15% of annual outpatient cases, in our experience.
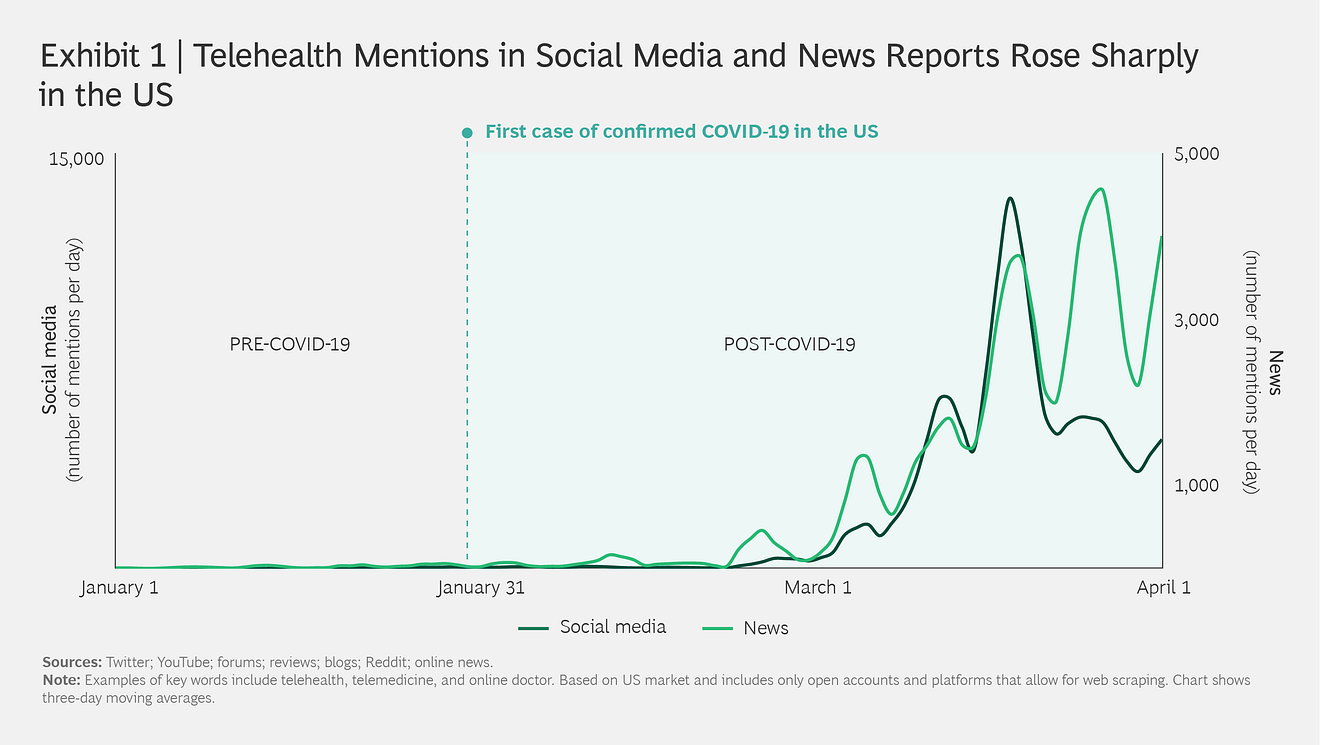
On the basis of early indicators, both clinicians and patients see clear benefits arising from new models of care, especially in the current environment. In the US, patient interest in digital platforms is remarkably high-for instance, mentions of “telehealth” in social media and news reports increased significantly in March. (See Exhibit 1.) The pandemic has also enabled virtual providers to reach new demographics, such as those older than age 60. A key benefit for clinicians is less exposure to infection-which is especially critical as the COVID-19 crisis continues. Moreover, the reduction in travel to the office allows clinicians to make better use of their time.
The Elements of the New Paradigm
Looking across world-leading organizations, we have identified six priority levers that health systems can apply in order to transition to a fundamentally different paradigm of outpatient care delivery, for all types of outpatient encounters. Some levers are specific to initial diagnosis or chronic disease management, while others are applicable to multiple care pathways. (See Exhibit 2.) Applied in combination, the levers could improve productivity by as much as 30% to 40% while maintaining quality and outcomes.
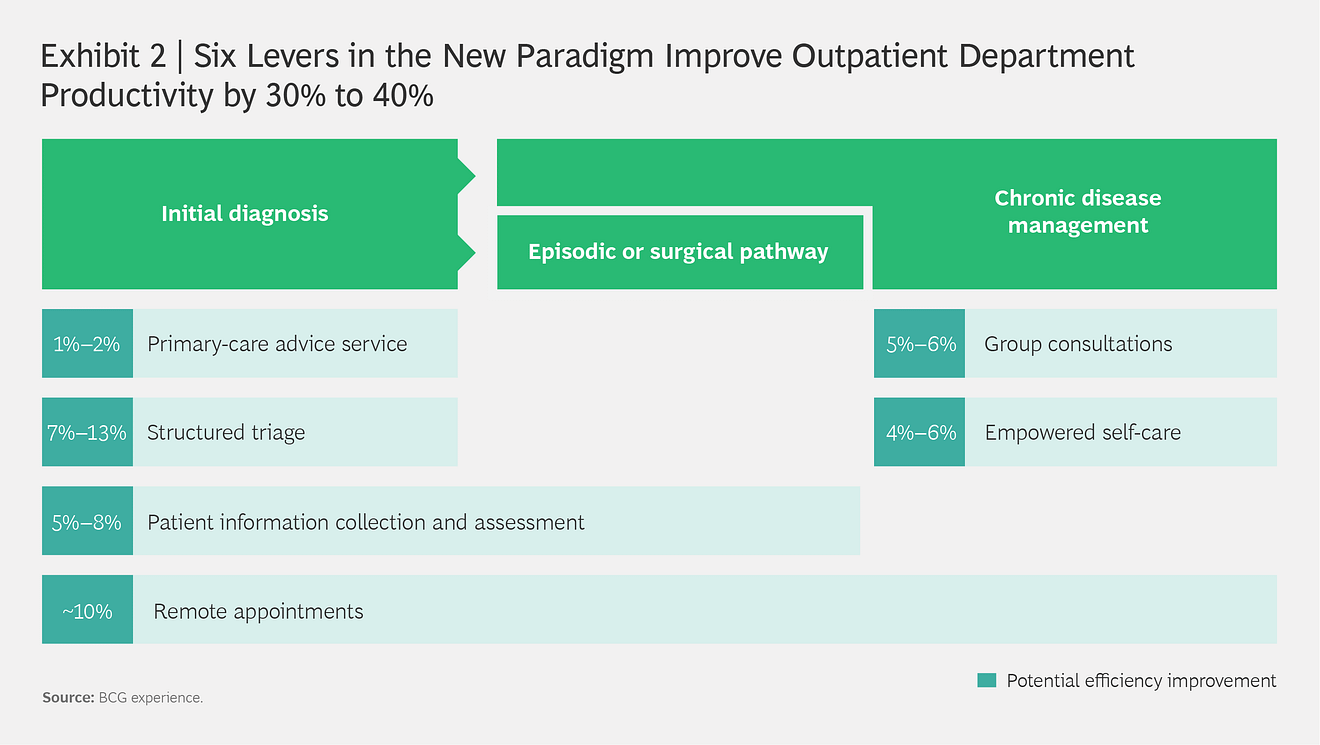
- Primary-Care Advice Service
- Structured Triage
- Patient Information Collection and Assessment
- Remote Appointments
- Group Consultations
- Empowered Self-Care
Primary-Care Advice Service. This is a live messaging service that allows primary care practices to send queries about patients to specialists and receive recommendations in response. By expanding the capabilities of primary care practices, the service could reduce the number of inappropriate outpatient referrals.
Structured Triage. A triage process for all appointments has several benefits. It ensures that referrals are appropriate, triggers any tests that must be done before an appointment (including those done with at-home test kits), and allows clinicians to assess the optimal mode of consultation (such as face to face, remote, or in a group setting). It also facilitates centralized scheduling of appointments. Organizations could augment manual efforts with algorithm-based triage (including self-triage). One health system found that deploying a triage chatbot on its website decreased calls by as much as 30%.
Patient Information Collection and Assessment. Health systems can use online forms (linked to electronic patient records [EPRs]) to capture patient history prior to the appointment, allowing clinicians to focus on diagnosis and treatment during patient visits. The assessment can include an algorithm-based “early warning” system that scrutinizes the information provided and ensures that patients undergo any necessary diagnostic tests before the appointment.
Remote Appointments. Conducting appointments via telephone and video has been the biggest shift in the care model during the COVID-19 crisis. A recent BCG survey found that more than 50% of patients in the US with unanticipated conditions are using remote care. Governments are taking steps to enable this-the German government, for example, has removed a reimbursement cap for primary care digital consultations (previously, only 20% of appointments with a specific provider could be remote per quarter). Moving face-to-face appointments to remote consultations improves access for patients, particularly those who live far away from the provider or are hampered by poor mobility. Remote consultations can also be more efficient, especially if the telemedicine interface is integrated into the EPR. Moreover, during the COVID-19 recovery period, the remote-first approach will help to minimize the risk of infection and protect vulnerable patients.
Group Consultations. By participating in group consultations for chronic disease management, patients can learn from and support one another. They can also gain access to a greater variety of health professionals, including physiotherapists and dieticians. Some organizations are providing these consultations in conjunction with online forums for patients.
Empowered Self-Care. Patient-initiated follow-ups and remote monitoring are particularly effective in enabling people with chronic diseases to manage their own condition on a daily basis and access specialist services when they need support. Rather than scheduling routine follow-up appointments for these patients, providers can set up advice hotlines and establish escalation points (such as a rise in blood pressure) that trigger a specialist consultation. The approach has been applied effectively across many types of services, including those for cancer and diabetes. Additionally, organizations can use remote monitoring to fundamentally change the model of care by enabling a specialist to review a patient’s progress daily. Remote monitoring can also be combined with at-home treatments (such as dialysis).
How to Initiate and Accelerate the Changes
To adopt the new paradigm for outpatient care, organizations should apply what they have learned during the crisis about new ways of working and delivering changes at COVID speed. Initiating the changes entails several imperatives:
- Lock in the changes already made. Use the major modifications that the COVID-19 response has triggered in your organization as the basis for getting started. To maintain the momentum for change, avoid the trap of looking for brand-new end-to-end solutions-a process that could take months. Instead, seek to lock in the changes you have already made to your systems and build on these modifications by learning from the success of other organizations.
- Win the hearts and minds of clinicians. Ensure buy-in from clinicians by measuring impact from the start. Demonstrate the value of new models of care through patient feedback, outcomes, and access metrics. Identify clinicians who can serve as pioneers to lead the transformation and leverage their support and advocacy.
- Set the right priorities. Focus first on the highest-impact specialties (those with the most clinical need and greatest level of activity). Start by applying a few key levers, such as remote appointments and triage, that open the door to other levers. For example, triage helps to enable group consultations and patient-initiated follow-ups. To avoid getting bogged down in time-consuming implementations, favor more generic, but scalable, solutions over initiatives tailored to individual specialties.
- Secure the necessary investment. Obtain the upfront funds required to implement new models of care by demonstrating the same-year payback. The return may be a lifeline to health systems that are under unprecedented financial strain. For instance, a recent BCG study found that almost two-thirds of US health and hospital systems face material financial risk owing to the burdens of the COVID-19 response.
To accelerate the changes, organizations should take the following steps:
- Scale rapidly. Start small, but once something works, scale quickly. Avoid getting stuck in “pilot purgatory.”
- Plan for the end state. The COVID-19 recovery is an opportunity to reimagine entirely new ways of working rather than simply evolving. That means designing new pathways instead of trying to execute the existing pathways differently. For example, redesign clinic templates and booking protocols for remote appointments rather than making tweaks to the current system for in-person appointments. To prevent slipping back to old ways of working by default, establish a formal approval process to restart face-to-face clinical service.
- Set up light-touch, robust governance. Delivering the changes at pace across all specialties will require senior sponsorship to enable new ways of working and remove roadblocks within the organization. Use weekly feedback loops with clinicians, supported by tracking of KPIs, to address snags and ensure delivery.
Health systems have a unique opportunity to use the momentum for change created by the COVID-19 crisis in order to accelerate the transformation of outpatient care. Tremendous potential exists to deploy precious resources more efficiently. Successful health systems will not only improve access to, and delivery of, outpatient care but also enhance their ability to sustain normal levels of care during future COVID-19 demand surges. Ultimately, the improvements will help systems achieve their overarching objective: better health outcomes at lower cost.
About the authors

Ben Horner; Managing Director & Partner; London

John Gooch; Managing Director & Senior Partner; London

Ania Labno; Managing Director & Partner; Chicago

John Gooch; Managing Director & Senior Partner; London
About Boston Consulting Group
Boston Consulting Group partners with leaders in business and society to tackle their most important challenges and capture their greatest opportunities. BCG was the pioneer in business strategy when it was founded in 1963. Today, we work closely with clients to embrace a transformational approach aimed at benefiting all stakeholders-empowering organizations to grow, build sustainable competitive advantage, and drive positive societal impact.
Our diverse, global teams bring deep industry and functional expertise and a range of perspectives that question the status quo and spark change. BCG delivers solutions through leading-edge management consulting, technology and design, and corporate and digital ventures. We work in a uniquely collaborative model across the firm and throughout all levels of the client organization, fueled by the goal of helping our clients thrive and enabling them to make the world a better place.
© Boston Consulting Group 2021. All rights reserved.
Originally published at https://www.bcg.com on July 21, 2020.
To download the PDF, open the URL below: