



This is a republication of the article “Data silos hold back healthcare”, with the title above, highlighting the message in question.
Experts call for Europe to do more to enable patients to share their health data
Science Business
By David Pringle
18 Aug 2022
This site version was edited by:
Joaquim Cardoso MSc.
health transformation . foundation
Data Driven Health Care Institute
August 22, 2022 (open health)
Europe is falling behind the US in harnessing patients’ data to improve healthcare.
That was the stark message from expert speakers in a panel discussion on data bottlenecks in healthcare at the EuroScience Open Forum (ESOF) held in July in Leiden.
“Unfortunately, the US is developing much faster and removing [the] barriers much faster than us Europeans,” Vincent Keunen, CEO and co-founder of Andaman 7, said during the discussion, which was organised by Science|Business.
“And that is without abusing privacy of patients too, so we really should learn a lot from them.”
Start-up Andaman7 provides patients with software they can use to manage and share their health data.
Although it is based in Belgium, Andaman7’s user base is mostly in the US where healthcare data is far more standardised and, therefore, more portable than in Europe.
Keunen explained that the Obama administration made the use of standard electronic healthcare record formats by healthcare providers a pre-requisite for reimbursement from federal funds.
… the Obama administration made the use of standard electronic healthcare record formats by healthcare providers a pre-requisite for reimbursement from federal funds.
… in the US …healthcare data is far more standardised and, therefore, more portable than in Europe.
As a result, patients being treated by 10,000 US hospitals (85% of the total) can download their data and share it with researchers, if they wish, he added.
“It took two years, but all the software is now compatible with one of those standards,” usually the FHIR (Fast Healthcare Interoperability Resources) standard, Keunen told the event.
“It took two years, but all the software is now compatible with one of those standards,” usually the FHIR (Fast Healthcare Interope…
“That was the first step, the technology was there. But there was still a lot of resistance from many layers.”
Under pressure from patient associations, the US government followed up by introducing a law to prevent so-called information blocking by some of the actors in the value chain, Keunen added.
Under pressure from patient associations, the US government followed up by introducing a law to prevent so-called information blocking by some of the actors in the value chain,
Other speakers warned that Europe is also moving slower than other regions to act on so-called real-world evidence about the efficacy of treatments.
Elke Grooten, Head of EU Relations at pharmaceutical company Novartis, said:
“If you look at other regions, like the US… but also Japan, even to a certain extent in China, the use of real-world evidence, in addition to the traditional clinical trials for the approval of treatments, is much more advanced.”
“If you look at other regions, like the US… but also Japan, even to a certain extent in China, the use of real-world evidence, in addition to the traditional clinical trials for the approval of treatments, is much more advanced.”
Novartis has found that in certain areas, such as gene therapies, rare diseases, sickle cell disease and cancer, real-world evidence collected in Europe has enabled it to gain approval for treatments in other regions.
Novartis has found that in certain areas, such as gene therapies, rare diseases, sickle cell disease and cancer, real-world evidence collected in Europe has enabled it to gain approval for treatments in other regions.
“But still in Europe, the European Medicines Agency, the regulators are asking us to do the traditional clinical trials,” Grooten added, which means “systematically treatments get approved much later in Europe than in other regions.”
“But still in Europe, the European Medicines Agency, the regulators are asking us to do the traditional clinical trials,” …which means “systematically treatments get approved much later in Europe than in other regions.”
Structure of the publication:
- Understanding the whole patient journey for each disease
- Calls for change are getting louder
- Can Europe move quicker?

Understanding the whole patient journey for each disease
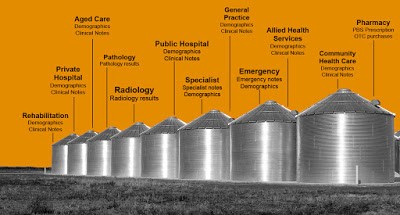
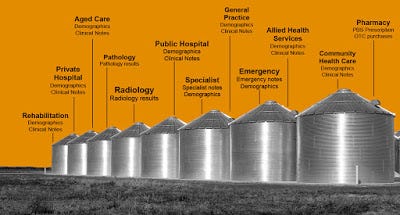
One of the challenges facing pharmaceuticals companies is they don’t know the context in which their treatments are being used.
They only have data on their “specific treatment and not what happens before and after,” Grooten noted.
“The true value of doing this right and breaking down the silos is that by understanding better the patients’ journeys collectively, we can actually come with better treatments and better interventions.”
They only have data on their “specific treatment and not what happens before and after,” …
In the EU, the General Data Protection Regulation (GDPR) is supposed to give citizens greater control over the usage of their data in a consistent way across the bloc.
However, in practice, the GDPR has been implemented (and enforced) somewhat differently in different countries, creating legal uncertainty that can result in lawyers erring on the side of caution.
For Novartis, the decision about where to conduct international clinical trials can often be determined by legal factors, as much as medical factors.
“When you decide… in which countries your experimental treatment becomes available for patients that might be helped by it, it’s done at a lawyer’s desk, when they compare which countries have a similar implementation of the GDPR,” Grooten explained.
However, there are some signs that key actors are becoming more comfortable with GDPR and its implications for medical research.
In universities, there has been a massive improvement over the past two years, according to Carl Johan Sundberg, Professor at the Karolinska Institutet, as healthcare researchers have scrambled to respond the pandemic.
However, he noted that other parts of the ecosystem, including hospitals and companies, still frequently cite legal concerns as a reason for not sharing data.
“The central governments in the countries and at the European level should simply provide strong guidelines,” he suggested.
In universities, there has been a massive improvement over the past two years…
However, … other parts of the ecosystem, including hospitals and companies, still frequently cite legal concerns as a reason for not sharing data.
“The central governments in the countries and at the European level should simply provide strong guidelines,” …
The Karolinska Institutet is developing a large computerised system into which patients can input their individual healthcare history via a tablet or computer.
Sundberg said the system now encompasses 15,000 tentative questions, which it could ask patients, depending on the information they provide.
“We’re now studying it in clinical trials and see that it’s massively better than what’s documented in the electronic health record systems in the same patients,” he added.
“So we need to move into developing such systems that collect and structure data because then we can do deeper analytics and that will be I think a game changer.”
“So we need to move into developing such systems that collect and structure data because then we can do deeper analytics and that will be I think a game changer.”
Sundberg noted that today patient data is often incomplete and unstructured in the form of prose.
“The text can be informative, of course, but it would be extremely advantageous if the data was already structured for future analytics,” he said.
“In addition to that, there’s a lot of erroneous entries… One reason might be the time pressure, and another reason might be the fact that it pays off to have a more severe diagnosis than the patient really has,” he added, noting that healthcare reimbursement systems can encourage this kind of misrepresentation.
“The text can be informative, of course, but it would be extremely advantageous if the data was already structured for future analytics,” he said.
Calls for change are getting louder
Citing opinion polls, the speakers argued that most patients are comfortable sharing their health data, as long as they retain control and the information is used to improve care and treatment.
Such sentiments may have been amplified by the experience of the COVID-19 pandemic.
As that crisis put healthcare systems in the spotlight, their deficiencies became apparent to citizens.
“In Sweden, it was quite obvious that the population actually thought that we had better control of our data than we do,” Anna Nilsson Vindefjärd, Secretary General of Research!Sweden, told the ESOF event.
“The pandemic actually made it visible to the population, that we do not have good interoperability.”
“The pandemic actually made it visible to the population, that we do not have good interoperability.”
One of the legal and ethical challenges is determining who exactly should control the data being generated by increasingly digitised healthcare systems.
Addressing the question of ownership gives rise to some delicate ethical considerations.
While patients increasingly take the “my body, my data” view, total transparency could lead to considerable anxiety and even harm, Vindefjärd noted.
“For the people in healthcare, for the professionals, they will have a lot of new information, maybe on the factor that this patient is high-risk for this typical disease, but there’s no cure for that disease,” Vindefjärd explained.
“At what percentage should that person tell the patient about it or not?”
There is also the question of how to communicate with patients in cases where treatments are available, but are beyond the budget of the national healthcare system
Addressing the question of ownership gives rise to some delicate ethical considerations.
While patients increasingly take the “my body, my data” view, total transparency could lead to considerable anxiety and even harm …
In Sweden, there are growing calls for guidelines on such matters, ideally developed by a professional committee on ethics working together with patient representatives.
Vindefjärd also made the case for investing more in training healthcare professionals in how to manage and analyse data, using artificial intelligence and other advanced tools.
“There are very few people at this point that are able to do that,” she noted.
While the private sector can outbid the public sector to recruit data specialists, “healthcare really needs these people in order to work with the data and have it in clinical research…
So there’s a need for universities to step in and actually create much more education, when it comes to healthcare data and how that is used in a better way.”
Vindefjärd also made the case for investing more in training healthcare professionals in how to manage and analyse data, using artificial intelligence and other advanced tools.
So there’s a need for universities to step in and actually create much more education, when it comes to healthcare data and how that is used in a better way.”
Can Europe move quicker?
Well aware of the importance of data sharing across the economy, the European Commission is developing so-called common data spaces covering different sectors.
These data spaces will encompass EU-wide mechanisms and standards designed to enable data to be shared between the public and private sectors and academia.
One of the first to be developed is likely to be the European Health Data Space (EHDS), which is earmarked to be fully up and running by 2025.
The speakers were hopeful that the EHDS will improve interoperability and give greater assurance to actors concerned about the legal subtleties.
However, Grooten of Novartis warned there are already signs that the EHDS is being used as an excuse to delay some actions, such as the increased use of real-world evidence, which can be implemented today.
“They say: let’s wait until the European health data space has been adopted,” she said. “Hopefully we won’t have too much of that.”
However, Grooten of Novartis warned there are already signs that the EHDS is being used as an excuse to delay some actions, such as the increased use of real-world evidence, which can be implemented today.
Keunen of Andaman7 described the EHDS as a very good idea, but he expressed concern about the timing. “Let’s hope that it gets implemented fast — and fast is not 2025.”
He called for all European users of healthcare data, such as hospitals and clinics, to be required to adopt the FHIR standard “for all the software being used in Europe, with fines if there is information blocking,” he contended.
“When I talk to people from the European Commission, they tend to say, well, it’s a national competency…each country has to decide for themselves. It’s never going to work if we leave it like that.”
He called for all European users of healthcare data, such as hospitals and clinics, to be required to adopt the FHIR standard “for all the software being used in Europe, with fines if there is information blocking,” he contended.
Originally published at https://sciencebusiness.net.
NAMES MENTIONED
Vincent Keunen, CEO and co-founder of Andaman 7,
Elke Grooten, Head of EU Relations at pharmaceutical company Novartis, said: “
Carl Johan Sundberg, Professor at the Karolinska Institutet,
Anna Nilsson Vindefjärd, Secretary General of Research!Sweden,







