A similar strategy, which recommended dose fractionation down to one fifth of the standard dose, worked in 2016–2018 for yelow fever, in Angola; the Democratic Republic of Congo , and subsequently in Brazil.
Nature Medicine
Benjamin J. Cowling; Wey Wen Lim & Sarah Cobey
Published: 05 July 2021
Credit to the image on the top: the medicine maker
To the Editor
COVID-19 continues to pose a major threat to public health.
Public-health and social measures have been implemented to control transmission, but they are emergency measures that are difficult to sustain in the longer term.
There are now 15 vaccines against COVID-19 being used worldwide. However, shortages in the supply of vaccines have been a particular problem for low-income countries, which have collectively received only 0.2% of all vaccines delivered worldwide for approximately 10% of the world’s population.
Fractionation of vaccine doses (Fig. 1) is a potential solution to this global shortage of vaccines that has not been given sufficient attention and consideration.
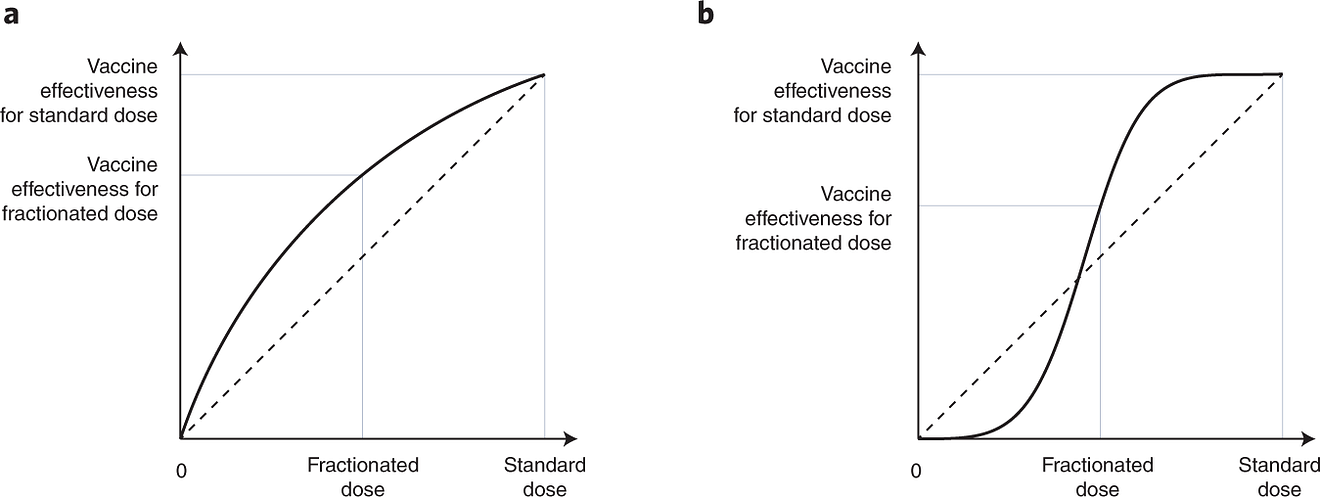
a, Solid line indicates a scenario in which there is a concave relationship between vaccine efficacy (vertical axis) and dosage (horizontal axis), whereby a fractionated dose (e.g., approximately half of a standard dose) could provide considerably more than half the effectiveness of the standard dose; the dashed diagonal line is included for reference. If the concave relationship holds, it indicates that providing half doses to a certain number of people could provide a greater level of population immunity than would providing standard doses to half as many people. For reference, the population immunity conferred by vaccination could be estimated via the vaccination coverage multiplied by vaccination effectiveness.
b, Another scenario in which very low fractionated doses might not provide any clinical benefit, but fractionation would still provide population benefits above a certain threshold. Here, the solid line crosses the diagonal dashed line at doses approaching half a standard dose, and at the fractionated dose indicated (approximately half a standard dose), there would be an advantage for population immunity to use half doses.
In 2015, emergency vaccination against yellow fever was needed to mitigate epidemics in Angola and the Democratic Republic of Congo.
However, there were limited supplies of the vaccine and there was a 6-month minimum manufacturing process.
The World Health Organization’s Strategic Advisory Group of Experts on Immunization reviewed evidence on the immunogenicity and safety of fractional dosing of vaccines against yellow fever and recommended dose fractionation down to one fifth of the standard dose.
- This was put into practice in Angola and the Democratic Republic of Congo in 2016, with millions vaccinated with the fractional dose,
- and was subsequently put into practice in Brazil in 2017–2018 (ref. ).
Fractional dosing was predicted to substantially reduce population infection attack rates and save lives.
Vaccine-dose fractionation has also been recommended by the World Health Organization for inactivated poliovirus vaccines and meningococcal conjugate vaccines as an alternative mass-vaccination strategy, particularly when vaccine shortages occur during outbreaks in resource-limited locations.
Dose-finding studies indicate that fractional doses of mRNA vaccines could still elicit a robust immune response to COVID-19. In a non-randomized open-label phase 1/2 trial of the BNT162b2 vaccine, doses as low as one third (10 μg) of the full dose produced antibody and cellular immune responses comparable to those achieved with the full dose of 30 μg (ref. ). Specifically, the geometric mean titer of neutralizing antibodies 21 days after the second vaccine dose was 166 for the group that received 10 μg, almost the same as the geometric mean titer of 161 for the group that received 30 μg, and 63 days after the second dose, these titers were 181 and 133, respectively. For the mRNA-1273 vaccine, a dose of 25 μg conferred geometric mean PRNT 80 titers (the inverse of the concentration of serum needed to reduce the number of plaques by 80% in a plaque reduction neutralization test) of 340 at 14 days after the second dose, compared with a value of 654 for the group that received the standard dose of 100 μg (ref. ). According to the model proposed by Khoury et al., if vaccine efficacy at the full dose is 95%, a reduction in dose that led to as much as a halving in the post-vaccination geometric mean titer could still be in the range of 85–90%. Although other components of the immune response may also contribute to efficacy, these dose-finding data are at least indicative of the potential for further exploration of fractionation as a dose-sparing strategy. Durability of responses after fractional doses should also be explored.
We are aware of only one trial reporting data on the clinical efficacy of a fractionated dosing strategy for COVID-19, which was a trial of the AZD1222 vaccine in the UK. As part of a larger multicenter trial, Voysey et al. reported a vaccine efficacy of 90% (67–97%) among a subgroup of participants who were primed with a half dose instead of a full dose, followed by a full-dose boost after a median of 12 weeks. Although only a small number of participants were included in this subgroup, the lower bound of 67% for the efficacy estimate is very reassuring.
Concerns about the evolution of vaccine resistance have been posited as a potential drawback of dose-sparing strategies. However, vaccines that provide protection against clinical disease seem to also reduce transmission, which indicates that expanding partial vaccination coverage could reduce the incidence of infection. As described in a recent paper, lower prevalence should slow, not accelerate, the emergence and spread of new SARS-CoV-2 variants. Within-host dynamics are unlikely to overcome these population-level effects. In contrast to some chronic infections, such as infection with human immunodeficiency virus, infection with SARS-CoV-2 in healthy people does not readily select for variants that escape the immune system. Such rapid selection has been reported only in immunocompromised people, who might have better access to vaccines if doses were fractionated in the general population. One other potential concern about fractionation would relate to vaccine hesitancy, if fractionated doses were viewed as inferior. However, the strategy of delaying the second dose of the vaccine applied in the UK and elsewhere has been well accepted as a strategy for providing at least partial protection to a greater number of people.
In conclusion, fractionated doses could provide a feasible solution that extends limited supplies of vaccines against COVID-19, which is a major challenge for low- and middle-income countries.
We identified several ongoing dose-finding studies on the ClinicalTrials.gov website that will provide important evidence to support fractionation policies.
Although most dose-finding studies focus on immune responses with relatively small sample sizes, larger trials to estimate the efficacy of fractionated doses would also be worthwhile.
The mRNA vaccines may be particularly suited for fractionation because of their higher levels of efficacy relative to those other vaccine types, while the favorable clinical-trial results on fractionation of the first dose of AZD1222 should encourage further investigation.
Even though some locations are reaching higher levels of vaccine coverage, many parts of the world with low vaccination rates could benefit from fractionation if it were determined to be an advantageous strategy.
Of course, vaccination rates are restricted not only by antigen supply but also by the availability of vaccinators and clinical supplies, such as syringes.
Nevertheless, antigen supply remains the greatest restriction for vaccines against COVID-19, and strategies that make the most of available antigen supply would maximize the number of lives saved by vaccination.
More generally, in future pandemics, researchers and clinicians involved in vaccine development should consider identifying the appropriate vaccine dosage that can save the most lives for a limited amount of antigen, rather than just a dosage that balances efficacy and reactogenicity for the individual person.
Acknowledgements Author information Ethics declarations
Acknowledgements
B.J.C. is supported by a fellowship award from the Research Grants Council of the Hong Kong Special Administrative Region (Project No. HKU SRFS2021–7S03).
Author information
Affiliations
- World Health Organization Collaborating Centre for Infectious Disease Epidemiology and Control, School of Public Health, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Hong Kong Special Administrative Region, Hong Kong, China
Benjamin J. Cowling & Wey Wen Lim - Laboratory of Data Discovery for Health Limited, Hong Kong Science and Technology Park, New Territories, Hong Kong Special Administrative Region, Hong Kong, China
Benjamin J. Cowling - Department of Ecology and Evolution, University of Chicago, Chicago, IL, USA
Sarah Cobey
Contributions
B.J.C. conceived of this Comment; B.J.C. wrote the original draft of the manuscript with contributions from all authors; and all authors reviewed and approved the final version of the manuscript.
References
See the original paper
Originally published at https://www.nature.com on July 5, 2021.
PDF version:
chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/viewer.html?pdfurl=https%3A%2F%2Fwww.nature.com%2Farticles%2Fs41591-021-01440-4.pdf&clen=830382&chunk=true