




NEJM
Véronique Bouvard, Ph.D., Suzanne T. Nethan, M.D.S., Deependra Singh, Ph.D., Saman Warnakulasuriya, Ph.D., Ravi Mehrotra, M.D., Ph.D., Anil K. Chaturvedi, M.P.H., Ph.D., Tony Hsiu-Hsi Chen, Ph.D., Olalekan A. Ayo-Yusuf, M.P.H., Ph.D., Prakash C. Gupta, Ph.D., Alexander R. Kerr, D.D.S., Wanninayake M. Tilakaratne, Ph.D., Devasena Anantharaman, Ph.D., David I. Conway, D.P.H., Ph.D., Ann Gillenwater, M.D., Newell W. Johnson, F.Med.Sci., Luiz P. Kowalski, M.D., Ph.D., Maria E. Leon, Ph.D., Olena Mandrik, Ph.D., Toru Nagao, D.D.S., Ph.D., D.M.Sc., Vinayak M. Prasad, M.B., B.S., Ph.D., Kunnambath Ramadas, M.D., Ph.D., Felipe Roitberg, M.D., Pierre Saintigny, M.D., Rengaswamy Sankaranarayanan, M.D., Alan R. Santos-Silva, D.D.S., Ph.D., Dhirendra N. Sinha, Ph.D., Patravoot Vatanasapt, M.D., Rosnah B. Zain, M.D.C., and Béatrice Lauby-Secretan, Ph.D.
October 18, 2022
Executive Summary by:
Joaquim Cardoso MSc.
health transformation — institute for research, strategy and advisory
October 26, 2022
Overview
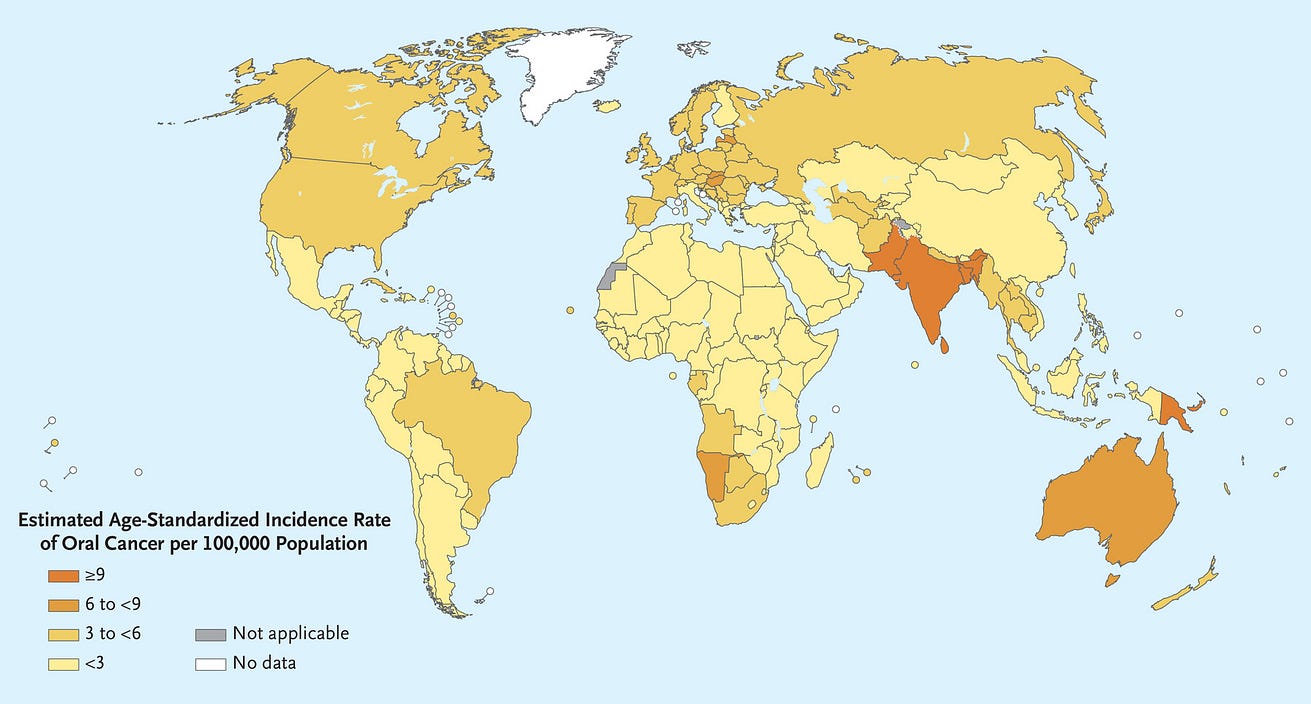
- In 2020, cancer of the lip and oral cavity was estimated to rank 16th in incidence and mortality worldwide and was a common cause of cancer death in men across much of South and Southeast Asia and the Western Pacific 1 (Figure 1).
[Figure 1 — Estimated Age-Standardized Incidence of Lip and Oral Cavity Cancers (2020).]
- A wide range of genetic, environmental, and behavioral factors contribute to the risk of oral cancer.2 Risks are dominated by tobacco, both smoked and smokeless, and heavy alcohol consumption.
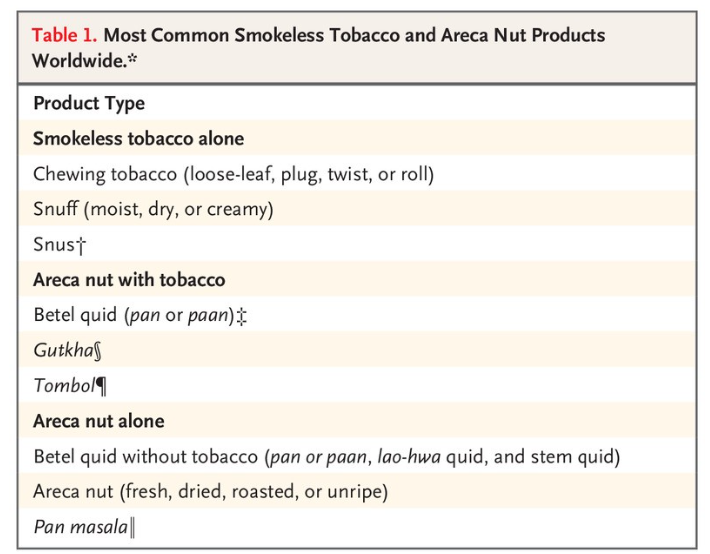
- In Southeast Asia and the Western Pacific Islands, where the incidence of oral cancer is high, the major risk factors are use of smokeless tobacco and areca nut products (including betel quid)3 (Table 1).4
- A small percentage of oral cancer worldwide (approximately 2%) is caused by human papillomavirus infection, primarily HPV16.5
- From September through December 2021, the International Agency for Research on Cancer (IARC) convened a working group of 25 scientists (all of whom are coauthors of this article) from 14 countries to evaluate the body of evidence on primary and secondary prevention of oral cancer.
- The working group reviewed all relevant published studies and evaluated the evidence according to the updated preambles of the IARC Handbooks of Cancer Prevention.6–8
- The preambles describe the objectives and scope of the program, general principles and procedures, and scientific review and evaluations.
- In addition, to strengthen the current published evidence with respect to areca nut products, the working group performed primary analyses of unpublished data from large studies.
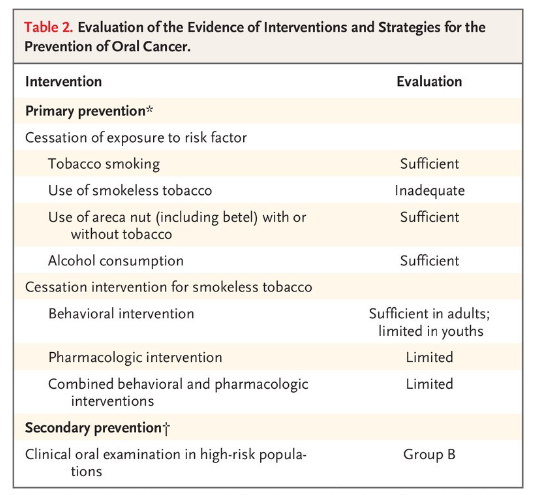
- Presented here is a brief overview of the studies that were reviewed and the outcomes of the evaluation process (Table 2)
For other sections:
See the original publication
Discussion and Conclusions
In this first evaluation of oral cancer prevention by the IARC Handbooks program, the working group found that tobacco smoking and alcohol consumption are the main drivers of oral cancer in most countries.
- However, the use of smokeless tobacco and chewing of areca nut products are the leading causes in many countries, especially in South and Southeast Asia and in the Western Pacific Islands.
- In these areas, the use of products (which may contain smokeless tobacco only, areca nut only, or both) vary widely in their nature and toxicity profile.
- In the available studies, a lack of detail regarding the composition of these products posed a challenge for the interpretation and evaluation of the current evidence.
Cessation of tobacco smoking and alcohol consumption has a preventive effect on the incidence of oral cancer and probably also decreases the risk of oral potentially malignant disorders. In addition, smoking cessation has many other health benefits.
- Given that the combined effect of tobacco smoking and alcohol consumption is greater than multiplicative, smoking cessation reduces the risk of oral cancer in persons who continue drinking alcohol.
- Similarly, the benefits of cessation in the use of areca nut products with or without tobacco have been established.
In reaching these conclusions, the working group considered that products vary substantially in composition, both within and among countries, and elected to evaluate jointly all products containing areca nut.
- Given interaction effects, large risk reductions would also be expected after smoking cessation in users of these products.
- Evidence for the benefits of cessation in the use of smokeless tobacco alone was inadequate because of the lack of studies in relevant geographic areas.
The effect of primary interventions for cessation of use of these products is specific to the country, culture, age, and sex of the target population.
- Very few studies were available in populations that commonly use areca nut with tobacco; therefore, the evaluations were limited to cessation of smokeless tobacco alone.
- As compared with adults, youth who initiate the use of smokeless tobacco often do not perceive tobacco as harmful and have high receptivity to tobacco advertising.
- Thus, it is important that education about harms of using these products focus on youths.
Clinical oral examination enables detection of oral cancer and oral potentially malignant disorders relatively early in their evolution.
- Currently, no better screening alternative exists, although research into biomarkers in saliva, blood, and breath is burgeoning.
- The highly variable natural history of oral potentially malignant disorders at the individual level poses a challenge in extrapolating data to important end points such as mortality.
- Evidence is still lacking with respect to whether adjunctive optical techniques or biomarkers can reduce false positive screening results.51
Our evaluation of the potential for clinical oral examination to reduce oral cancer mortality applies to high-risk persons only.
- Its effect in the general population cannot be established on the basis of current evidence.47
- Screening performed by trained primary health care workers in low-resource settings has shown good results on early disease detection.
- Opportunistic screening in dental practices in locations where health care resources are high may also be effective, although the evidence is scarce.52
- The use of risk-based models for screening could be an appropriate approach for communities with a high incidence of oral cancer, with the acknowledgment that selection of participants is challenging from a programmatic perspective.
Screening performed by trained primary health care workers in low-resource settings has shown good results on early disease detection.
Opportunistic screening in dental practices in locations where health care resources are high may also be effective, although the evidence is scarce.52
The use of risk-based models for screening could be an appropriate approach for communities with a high incidence of oral cancer, with the acknowledgment that selection of participants is challenging from a programmatic perspective.
This review highlighted the paucity of data in the area of oral cancer prevention and calls for additional research in all aspects of such preventive work.
- Nonetheless, the working group established that cessation of tobacco smoking, alcohol consumption, and areca nut use will contribute to significant reductions in the risk of oral cancer.
- Such measures will also contribute to the overall objective of the resolution on oral health adopted by the World Health Assembly in May 2021 to control and prevent oral diseases, including oral cancer, by 2030.53
This review highlighted the paucity of data in the area of oral cancer prevention and calls for additional research in all aspects of such preventive work.
Nonetheless, the working group established that cessation of tobacco smoking, alcohol consumption, and areca nut use will contribute to significant reductions in the risk of oral cancer.
Authors Affiliations
From the International Agency for Research on Cancer (V.B., S.T.N., D.S., R.S., B.L.-S.), and INSERM 1052, Centre National de la Recherche Scientifique 5286, Centre de Recherche en Cancérologie de Lyon, Université Claude Bernard Lyon 1, and the Department of Medical Oncology, Centre Léon Bérard (P.S.) — all in Lyon, France; the Collaborating Centre for Oral Cancer of the World Health Organization (WHO) (S.W.) and the Faculty of Dentistry, Oral, and Craniofacial Sciences (N.W.J.), King’s College London, London, the University of Sheffield School of Health and Related Research, Sheffield (O.M.), and the School of Medicine, Dentistry, and Nursing, University of Glasgow, Glasgow (D.I.C.) — all in the United Kingdom; Center for Health, Innovation, and Policy Foundation and Rollins School of Public Health, Emory University, Atlanta (R.M.); the Division of Cancer Epidemiology and Genetics, National Cancer Institute, National Institutes of Health, Bethesda, MD (A.K.C.); the Institute of Epidemiology and Preventive Medicine, National Taiwan University, Taipei (T.H.-H.C.); Sefako Makgatho Health Sciences University, Ga-Rankuwa, and the School of Health Systems and Public Health, University of Pretoria, Pretoria — both in South Africa (O.A.A.-Y.); Healis Sekhsaria Institute for Public Health (P.C.G.) and Preventive Oncology, Karkinos Healthcare (R.S.), Navi Mumbai, Rajiv Gandhi Centre for Biotechnology, Thiruvananthapuram (D.A.), Regional Cancer Centre, Trivandrum (K.R.), and the School of Preventive Oncology, Patna (D.N.S.) — all in India; New York University College of Dentistry, New York (A.R.K.); University of Peradeniya, Peradeniya, Sri Lanka (W.M.T.); the Faculty of Dentistry, University of Malaya, Kuala Lumpur (W.M.T., R.B.Z.), and MAHSA (Malaysian Allied Health Sciences Academy) University, Bandar Saujana Putra (R.B.Z.) — both in Malaysia; M.D. Anderson Cancer Center, Houston (A.G.); Griffith University Gold Coast, Southport, QLD, Australia (N.W.J.); University of São Paulo Medical School and A.C. Camargo Cancer Center (L.P.K.), São Paulo, and Piracicaba Dental School, University of Campinas, Campinas (A.R.S.-S.) — all in Brazil;
the Department of Maxillofacial Surgery, School of Dentistry, Aichi Gakuin University, Nisshin, Japan (T.N.); WHO, Geneva (V.M.P., F.R.); and the Department of Otorhinolaryngology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand (P.V.).
Dr. Lauby-Secretan can be contacted at secretanb@iarc.who.int or at the International Agency for Research on Cancer, Evidence Synthesis and Classification Branch, 150 Albert Thomas, 69372 Lyon Cedex 8, France.
References
See the original publication
Originally published at https://www.nejm.org.
About the authors & affiliations
- Véronique Bouvard, Ph.D.,
- Suzanne T. Nethan, M.D.S.,
- Deependra Singh, Ph.D.,
- Saman Warnakulasuriya, Ph.D.,
- Ravi Mehrotra, M.D., Ph.D.,
- Anil K. Chaturvedi, M.P.H., Ph.D.,
- Tony Hsiu-Hsi Chen, Ph.D.,
- Olalekan A. Ayo-Yusuf, M.P.H., Ph.D.,
- Prakash C. Gupta, Ph.D.,
- Alexander R. Kerr, D.D.S.,
- Wanninayake M. Tilakaratne, Ph.D.,
- Devasena Anantharaman, Ph.D.,
- David I. Conway, D.P.H., Ph.D.,
- Ann Gillenwater, M.D.,
- Newell W. Johnson, F.Med.Sci.,
- Luiz P. Kowalski, M.D., Ph.D.,
- Maria E. Leon, Ph.D.,
- Olena Mandrik, Ph.D.,
- Toru Nagao, D.D.S., Ph.D., D.M.Sc.,
- Vinayak M. Prasad, M.B., B.S., Ph.D.,
- Kunnambath Ramadas, M.D., Ph.D.,
- Felipe Roitberg, M.D.,
- Pierre Saintigny, M.D.,
- Rengaswamy Sankaranarayanan, M.D.,
- Alan R. Santos-Silva, D.D.S., Ph.D.,
- Dhirendra N. Sinha, Ph.D.,
- Patravoot Vatanasapt, M.D.,
- Rosnah B. Zain, M.D.C.,
- and Béatrice Lauby-Secretan, Ph.D.
About the Brazilian authors:
Felipe Roitberg, M.D.
Alan R. Santos-Silva, D.D.S., Ph.D.,
University of São Paulo Medical School and
A.C. Camargo Cancer Center (L.P.K.), São Paulo, and
Piracicaba Dental School,
University of Campinas, Campinas (A.R.S.-S.) — all in Brazil;
References
See the original publication
Originally published at https://www.nejm.org.
About the authors & affiliations
- Véronique Bouvard, Ph.D.,
- Suzanne T. Nethan, M.D.S.,
- Deependra Singh, Ph.D.,
- Saman Warnakulasuriya, Ph.D.,
- Ravi Mehrotra, M.D., Ph.D.,
- Anil K. Chaturvedi, M.P.H., Ph.D.,
- Tony Hsiu-Hsi Chen, Ph.D.,
- Olalekan A. Ayo-Yusuf, M.P.H., Ph.D.,
- Prakash C. Gupta, Ph.D.,
- Alexander R. Kerr, D.D.S.,
- Wanninayake M. Tilakaratne, Ph.D.,
- Devasena Anantharaman, Ph.D.,
- David I. Conway, D.P.H., Ph.D.,
- Ann Gillenwater, M.D.,
- Newell W. Johnson, F.Med.Sci.,
- Luiz P. Kowalski, M.D., Ph.D.,
- Maria E. Leon, Ph.D.,
- Olena Mandrik, Ph.D.,
- Toru Nagao, D.D.S., Ph.D., D.M.Sc.,
- Vinayak M. Prasad, M.B., B.S., Ph.D.,
- Kunnambath Ramadas, M.D., Ph.D.,
- Felipe Roitberg, M.D.,
- Pierre Saintigny, M.D.,
- Rengaswamy Sankaranarayanan, M.D.,
- Alan R. Santos-Silva, D.D.S., Ph.D.,
- Dhirendra N. Sinha, Ph.D.,
- Patravoot Vatanasapt, M.D.,
- Rosnah B. Zain, M.D.C.,
- and Béatrice Lauby-Secretan, Ph.D.
About the Brazilian authors:
Felipe Roitberg, M.D.
Alan R. Santos-Silva, D.D.S., Ph.D.,
University of São Paulo Medical School and
A.C. Camargo Cancer Center (L.P.K.), São Paulo, and
Piracicaba Dental School,
University of Campinas, Campinas (A.R.S.-S.) — all in Brazil;