




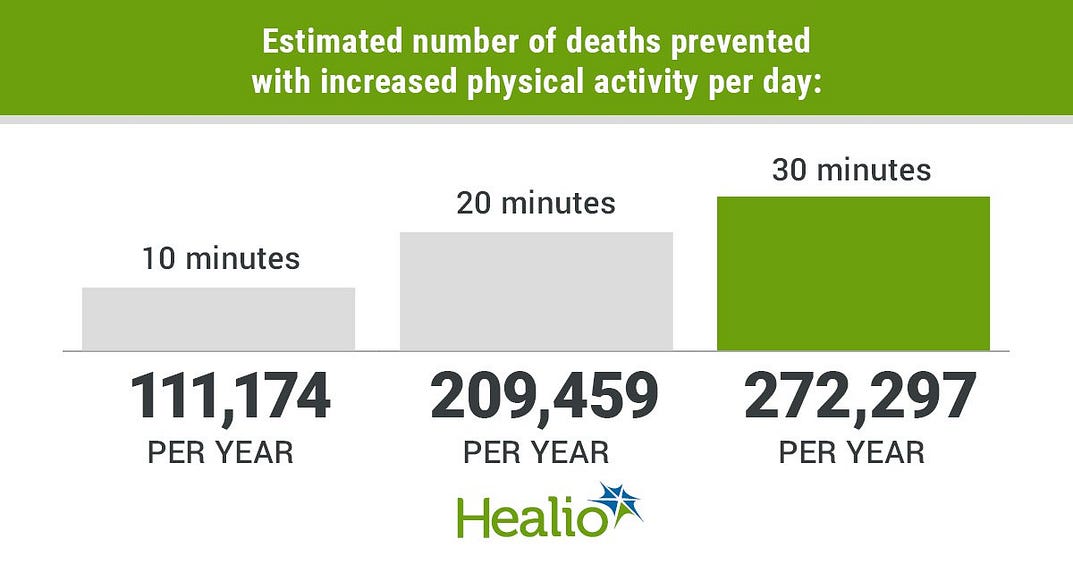
The benefits for 20 minutes/day are almost double, and 30 minutes/day higher.
The Hybrid Health Institute blog
Joaquim Cardoso MSc., Chief Editor
February 4, 2022
churchview medical practice
Adapted from the National Cancer Institute (US)
We know exercise is good for us.
And there is strong evidence that higher levels of physical activity are linked to lower risk of several types of cancer.
Now, a new study led by NCI researchers suggests that if adults were to increase moderate-to-vigorous exercise by a small amount, such as 10 minutes per day, an estimated 110,000 deaths could be prevented each year.
Key messages (by Joaquim Cardoso MSc.)
- Increasing MVPA by 10, 20, or 30 minutes per day was associated with a 6.9%, 13.0%, and 16.9% decrease in the number of deaths per year, respectively.
- Adding 10 minutes per day of physical activity resulted in an estimated 111 174 preventable deaths per year,
- with greater benefits associated with the addition of more physical activity (209 459 preventable deaths for 20 minutes
- and 272 297 preventable deaths for 30 minutes)
healio
This was the first study to estimate the number of preventable deaths through physical activity using accelerometer-based measurements among US adults while recognizing that increasing activity may not be possible for everyone (See below for the details about the Method).
Adapted from the National Cancer Institute (US)
https://www.linkedin.com/feed/update/urn:li:activity:6895496945423540224/
ORIGINAL PUBLICATION
Estimated Number of Deaths Prevented Through Increased Physical Activity Among US Adults
Jama Network
Pedro F. Saint-Maurice, PhD1; Barry I. Graubard, PhD1; Richard P. Troiano, PhD2; David Berrigan, PhD2; Deborah A. Galuska, PhD3; Janet E. Fulton, PhD3; Charles E. Matthews, PhD1
January 24, 2022.
Previous studies suggest that a substantial number of deaths could be prevented annually by increasing population levels of physical activity.1–3
However, previous estimates have relied on convenience samples,2,3 used self-reported physical activity data,1–3 and assumed relatively large increases in activity levels (eg, more than 30 minutes per day).1–3
The potential public health benefit of changing daily physical activity by a manageable amount is not yet known.
In this study, we used accelerometer measurements
(1) to examine the association of physical activity and mortality in a population-based sample of US adults and
(2) to estimate the number of deaths prevented annually with modest increases in moderate-to-vigorous physical activity intensity (MVPA).
Methods
This cohort study was approved by the National Center for Health Statistics Ethics Review Board.
This study used data from the National Health and Nutrition Examination Survey (NHANES), and written informed consent was obtained for all NHANES participants.
The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
The NHANES is a representative survey of the US civilian, noninstitutionalized population, including oversampling for non-Hispanic Black participants and Mexican American participants.
Race and ethnicity was determined by self-report and classified using preferred terminology from the National Center for Health Statistics as Mexican American, non-Hispanic Black, non-Hispanic White, or other.
Race and ethnicity was included in this study to better characterize the US population.
In 2003 to 2006, NHANES participants aged 6 years or older were asked to wear an accelerometer for 7 days.
For this study, we evaluated 4840 of 6355 adults aged 40 to 85 years or older with accelerometer data. The remaining 1515 individuals were excluded because they were not eligible or refused to participate in the monitoring protocol (853 [13%]), had monitors that malfunctioned or lost calibration (360 [6%]), or had no valid days with monitor data (302 [5%]).
Mortality follow-up was completed via National Death Index linkage through December 31, 2015.
We estimated MVPA by summing accelerometer minutes at or above an established cutpoint4 and creating 8 physical activity categories (0–19, 20–39, 40–59, 60–79, 80–99, 100–119, 120–139, or ≥140 minutes per day).
The number of deaths per year prevented with increased physical activity was estimated as the adjusted population attributable fraction (PAF)5 multiplied by the US population annual number of deaths for 2003 (for individuals aged 40–84 years).
To calculate the PAFs, we used population prevalence estimates and hazard ratios adjusted for age, sex, race and ethnicity, education level, body mass index (calculated as weight in kilograms divided by height in meters squared), diet, alcohol use, smoking status, and self-reported chronic conditions, mobility limitations, and general health.
Hazard ratios were estimated using Cox proportional hazard regression models, and the proportional hazards assumption was confirmed for our main exposure (ie, MVPA).
Counterfactuals for increased activity were set to 10, 20, and 30 minutes per day higher than participants’ observed values.
Those classified as frail6 or who required equipment to walk were assumed to be unable to increase their activity (eMethods in the Supplement); when PAFs were calculated, physical activity levels for these participants were held constant.
Data were analyzed with SAS version 9.4 (SAS Institute Inc), accounting for the NHANES complex sample design.
Results
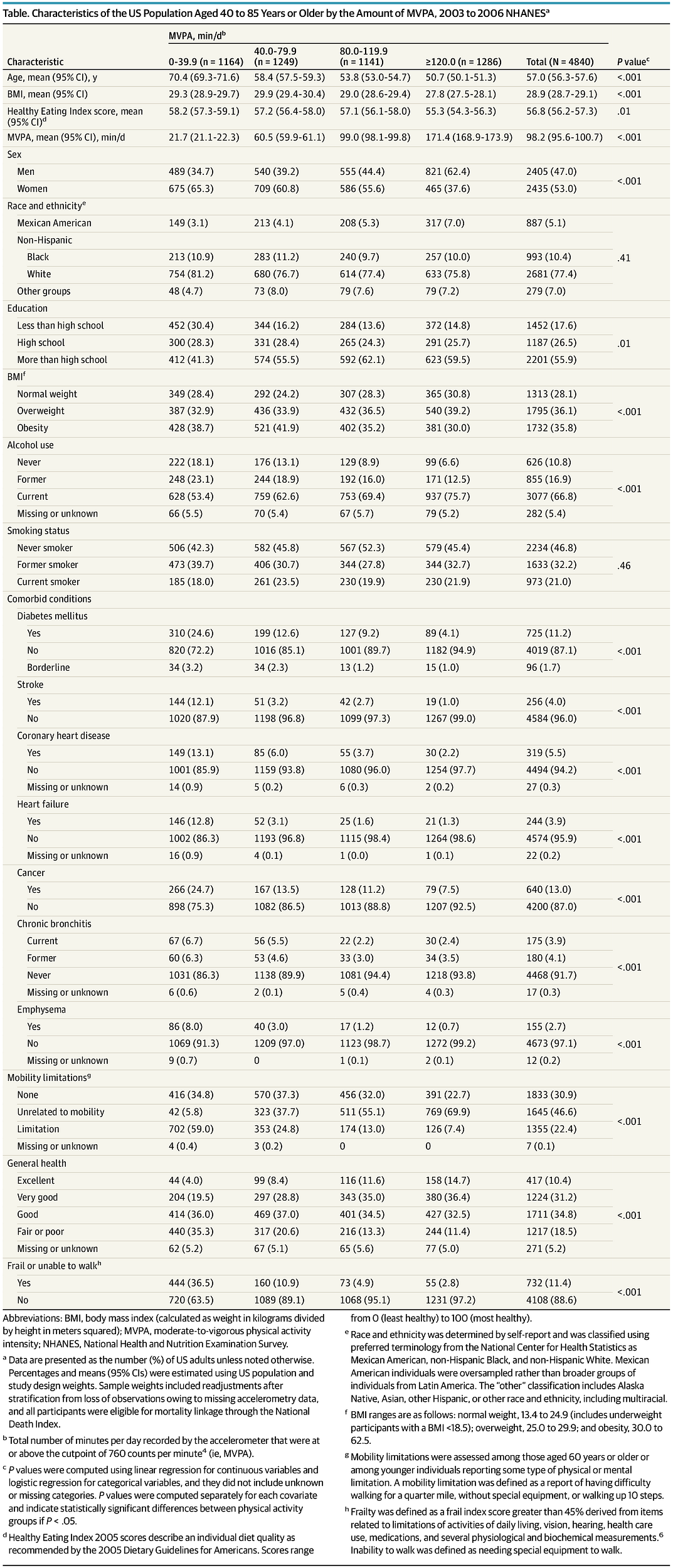
This analysis included 4840 participants. Of these, 2435 (53%) were women, 993 (10.4%) were non-Hispanic Black, and 887 (5.1%) were Mexican American (Table).
A total of 1165 deaths occurred during a mean (SEM) follow-up of 10.1 (0.1) years.
Adjusted hazard ratios changed from 0.69 to 0.28 across increasing activity categories (vs 0–19 minutes per day).
Hazard ratios used to generate the PAFs for the 8 activity categories were as follows: 1.00 (reference) for 0 to 19 (548 [7.9%]), 0.69 (95% CI, 0.55–0.85) for 20 to 39 (616 [10.0%]), 0.51 (95% CI, 0.42–0.63) for 40 to 59 (635 [11.8%]), 0.40 (95% CI, 0.29–0.55) for 60 to 79 (614 [12.7%]), 0.34 (95% CI, 0.25–0.47) for 80–99 (633 [14.4%]), 0.32 (95% CI, 0.21–0.48) for 100 to 119 (508 [12.1%]), 0.30 (95% CI, 0.19–0.48) for 120–139 (384 [9.3%]), and 0.28 (95% CI, 0.18–0.42) for 140 or more (902 [21.7%]) minutes per day.
The number of participants with frailty or needing special equipment was 280 (49.4%) for 0 to 19, 164 (26.3%) for 20 to 39, 94 (12.4%) for 40 to 59, 66 (9.5%) for 60 to 79, 42 (5.1%) for 80 to 99, 31 (4.7%) for 100 to 119, 20 (2.9%) for 120 to 139, and 35 (2.7%) for 140 or more minutes per day.
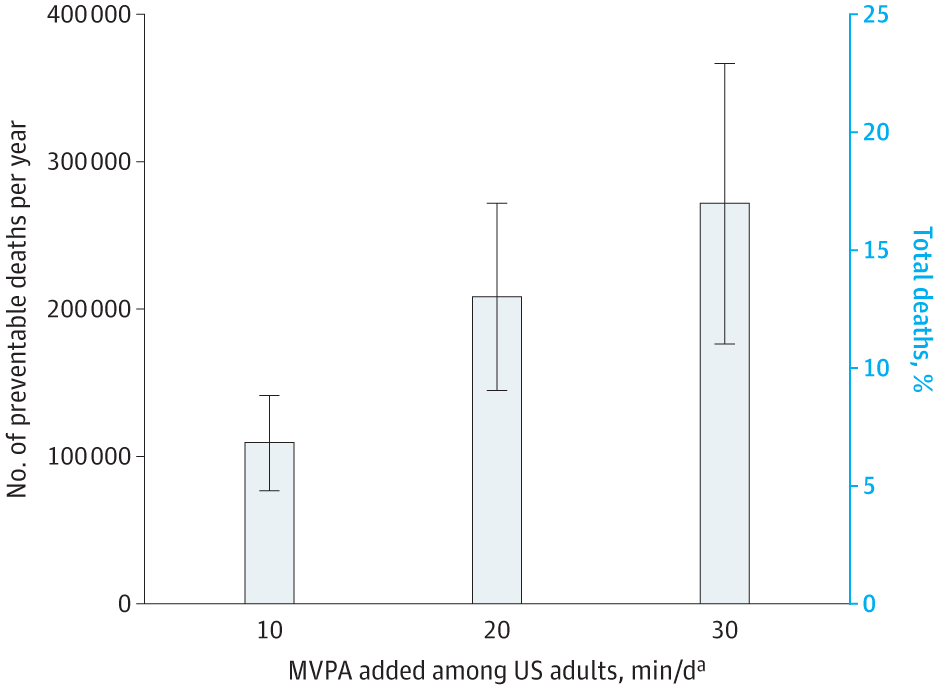
Increasing MVPA by 10, 20, or 30 minutes per day was associated with a 6.9%, 13.0%, and 16.9% decrease in the number of deaths per year, respectively.
- Adding 10 minutes per day of physical activity resulted in an estimated 111 174 preventable deaths per year (95% CI, 79 594–142 754),
- with greater benefits associated with the addition of more physical activity (209 459 preventable deaths [95% CI, 146 299–272 619] for 20 minutes
- and 272 297 preventable deaths [95% CI, 177 557–367 037] for 30 minutes) (Figure).
The PAFs indicate that the addition of 10 minutes per day of MVPA was associated with the prevention of 8.0% (95% CI, 6.0–10.0) of total deaths per year among men, 5.9% (95% CI, 2.0–9.8) among women, 4.8% (95% CI, 0.0–10.7) among Mexican American individuals, 6.1% (95% CI, 2.2–10.0) among non-Hispanic Black individuals, and 7.3% (95% CI, 5.3–9.3) among non-Hispanic White individuals.
Discussion
In this cohort study, we estimated that approximately 110 000 deaths per year could be prevented if US adults aged 40 to 85 years or older increased their MVPA by a small amount (ie, 10 minutes per day).
Similar benefits were observed for men and women and for Mexican American, non-Hispanic Black, and non-Hispanic White adults.
To our knowledge, this is the first study to estimate the number of preventable deaths through physical activity using accelerometer-based measurements among US adults while recognizing that increasing activity may not be possible for everyone.
However, 1 week of monitoring may not reflect changes in activity over time, and the observational study design limits the direct determination of causality.
These findings support implementing evidence-based strategies to improve physical activity for adults and potentially reduce deaths in the US.
About the authors and affiliations
Pedro F. Saint-Maurice, PhD1; Barry I. Graubard, PhD1; Richard P. Troiano, PhD2; David Berrigan, PhD2; Deborah A. Galuska, PhD3; Janet E. Fulton, PhD3; Charles E. Matthews, PhD1
1Division of Cancer Epidemiology and Genetics, National Cancer Institute, Rockville, Maryland
2Division of Cancer Control and Population Sciences, National Cancer Institute, Rockville, Maryland
3Division of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, Atlanta, Georgia
References and additional information
See the original publication.






