




This is an excerpt of the publication “McBeath, K.C.C., Angermann, C.E. & Cowie, M.R. Digital Technologies to Support Better Outcome and Experience of Care in Patients with Heart Failure. Curr Heart Fail Rep (2022). https://doi.org/10.1007/s11897-022-00548-z”.
The focus is on the topic above. For the full version of the original publication, please, refer to the second part of this post.
Authors
Current Heart Failure Reports
K. C. C. McBeath, C. E. Angermann & M. R. Cowie
29 April 2022
Excerpt by
Joaquim Cardoso MSc.
Health Revolution Institute
Digital Health Unit
May 1, 2022
Right Technology, Right patient, Right time: a Vision of the Future
Comparison of the traditional model with the modern model
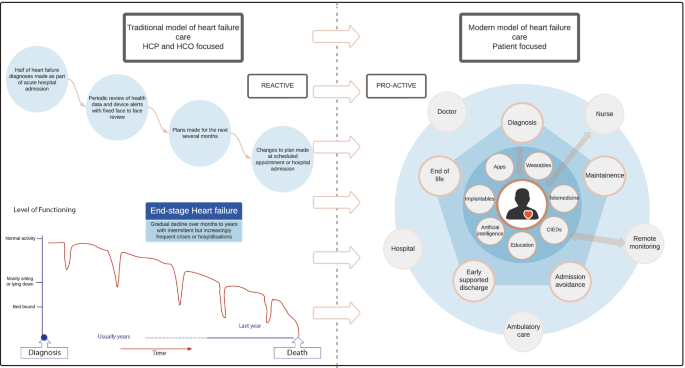
The contrast between the traditional model of heart failure care (left), with a modern digitally-supported patient-centric model of heart failure care (right).
- The traditional model uses fixed periodic review with a healthcare organisation (HCO) focus on reactive management of patient crises.
- The modern model of heart failure care uses digital technology to support patients at various stages of their heart failure illness, allowing dynamic management of issues as they arise.
Right Technology, Right patient, Right time: a Vision of the Future
The traditional model of HF care with periodic clinic review, using only data collected at that time by the healthcare team using “their” technologies, is likely to be replaced (or at least supplemented) by a more patient-centric approach.
Collecting data remotely provides “real” life data — which represent more than 99% of the time when patients are in their own environment — to be used in shared decision-making.
The traditional model of HF care with periodic clinic review, using only data collected at that time by the healthcare team using “their” technologies, is likely to be replaced (or at least supplemented) by a more patient-centric approach
Collecting data remotely provides “real” life data — which represent more than 99% of the time when patients are in their own environment — to be used in shared decision-making.
Shared decision-making requires a good working relationship between patient and HCP, as well as a patient who is adequately informed, educated and (therefore) motivated to make changes based on remote monitoring data.
Access to HCPs and systems will still be needed and must be available flexibly and at potentially short notice, but much of the routine processes of care can be supported by technology and RPM, freeing up time and bandwidth for members of the healthcare team to deal with the more complex, or nuanced, situations where human-to-human interaction adds more value.
In practice, digital remote technologies will support the key activities within the care pathway — ensuring rapid and accurate diagnosis, risk stratification and prognostication, therapeutic decision-making and tailored support including education and care.
Active shared decision-making between clinician and patient will decide which technology can best be used to achieve the shared goals, whether it is initial education and support to self-care, identification when another therapy may be beneficial, or helping the patient maintain stability with optimised quality of life at home, without the need to engage with the “official” healthcare system by attending clinic or being hospitalised.
Technology should provide closed-loop interactions with patients, offering advice on fluid intake, diuretic regime, exercise, necessity for blood tests and when to contact an HCP.
When patients require input from an HCP they deserve a tailored and responsive interaction based on multiple relevant data points and sources, with decision and sensemaking supported by digital tools (and likely artificial intelligence).
Clinical deterioration will be predicted and identified early using remote monitoring and stabilisation facilitated by appropriate escalation of therapy.
Admission to hospital will, of course, remain necessary for some patients, but early discharge will be supported with virtual wards (“hospital-at-home”) with monitoring pathways and rehabilitation facilitated remotely.
We highlight the differences between the traditional model of care and this more modern, digitally enabled approach to HF care in Fig. 1.
Conclusion
Digital technologies are already deeply embedded within all aspects of society, including health and healthcare.
HF care already relies on many of them, but the clinical pathways and treatment algorithms to successfully integrate digital technologies and decision support into the healthcare system are in their infancy.
Ultimately, digital technologies will become part of the “new normal”, being selected for use when they make sense and help patients and their HCPs achieve shared goals.
Digital technologies are already deeply embedded within all aspects of society, including health and healthcare.
HF care already relies on many of them, but the clinical pathways and treatment algorithms to successfully integrate digital technologies and decision support into the healthcare system are in their infancy.
Ultimately, digital technologies will become part of the “new normal”, …
Due consideration must be paid to ensuring the evidence base is robust, that data flows and human factors are considered, and that the digital technologies are co-designed and implemented to ensure a better outcome and experience of care.
Data should not be collected for its own sake — it must support better decision-making and more efficient care.
ORIGINAL PUBLICATION (full version)
Digital Technologies to Support Better Outcome and Experience of Care — in Patients with Heart Failure
Current Heart Failure Reports
K. C. C. McBeath, C. E. Angermann & M. R. Cowie
29 April 2022
ABSTRACT
Purpose of Review
In this article, we review a range of digital technologies for possible application in heart failure patients, with a focus on lessons learned.
We also discuss a future model of heart failure management, as digital technologies continue to become part of standard care.
Recent Findings
Digital technologies are increasingly used by healthcare professionals and those living with heart failure to support more personalised and timely shared decision-making, earlier identification of problems, and an improved experience of care.
The COVID-19 pandemic has accelerated the acceptability and implementation of a range of digital technologies, including remote monitoring and health tracking, mobile health (wearable technology and smartphone-based applications), and the use of machine learning to augment data interpretation and decision-making.
Much has been learned over recent decades on the challenges and opportunities of technology development, including how best to evaluate the impact of digital health interventions on health and healthcare, the human factors involved in implementation and how best to integrate dataflows into the clinical pathway.
Summary
Supporting patients with heart failure as well as healthcare professionals (both with a broad range of health and digital literacy skills) is crucial to success.
Access to digital technologies and the internet remains a challenge for some patients.
The aim should be to identify the right technology for the right patient at the right time, in a process of co-design and co-implementation with patients.
The aim should be to identify the right technology for the right patient at the right time, in a process of co-design and co-implementation with patients.
Introduction
Digital health encompasses the creation and practical use of computerised devices, methods and systems for health and healthcare [ 1].
It includes mobile health (mHealth: the use of mobile and wireless technologies to support achieving health objectives [ 2]), health information technology (IT), wearable devices and remote patient management (RPM).
Digital health is an integral part of the transformation of healthcare systems towards a more patient-centric preventive model, where resources are focused toward health maintenance rather than only on crisis management.
Digital health encompasses the creation and practical use of computerised devices, methods and systems for health and healthcare .
It includes: (1) mobile health (mHealth: the use of mobile and wireless technologies to support achieving health objectives ), (2) health information technology (IT), (3) wearable devices and (4) remote patient management (RPM).
The vision of a person-centred healthcare system is key to policy makers’ plans for a more modern, flexible and sustainable healthcare system [ 3, 4], where people living with (or at risk of) cardiovascular disease use a range of digital technologies to ensure optimal experience and outcome of health (and healthcare) decision-making, only interacting with the appropriate healthcare professionals when (and if) this is useful.
The vision of a person-centred healthcare system is key to policy makers’ plans for a more modern, flexible and sustainable healthcare system …
The implementation of digital systems in healthcare such as electronic medical records and e-prescribing has accelerated in recent years [ 5] but technologies to support health maintenance and healthcare decision-making (such as remote monitoring) have seen slower uptake.
The COVID-19 pandemic has triggered a rapid wave of adoption and greater acceptance of digital technologies by patients, healthcare professionals (HCP) and systems — a process often referred to as a “tech-celleration” — as change that was expected to take years occurred within a few weeks in response to the need for restricted face-to-face interaction [ 6 *].
This article reviews the lessons learned in the creation, assessment and implementation of digital health technologies for heart failure (HF) management, focusing on remote monitoring and devices to support and improve patient and HCP decision-making (remote patient management, RPM) compared with traditional HF care strategies (Fig. 1).
We also share our vision of the future, where the right tool is used at the right time and in the right place to enable optimal outcome and experience of care.
The contrast between the traditional model of heart failure care (left), with a modern digitally-supported patient-centric model of heart failure care (right).
- The traditional model uses fixed periodic review with a healthcare organisation (HCO) focus on reactive management of patient crises.
- The modern model of heart failure care uses digital technology to support patients at various stages of their heart failure illness, allowing dynamic management of issues as they arise.
Healthcare organisation focus is on pro-active health maintenance. HCP, healthcare professional; HCO, healthcare organisation; CIEDs, cardiac implantable electronic devices; Apps, smartphone applications
The traditional model uses fixed periodic review with a healthcare organisation (HCO) focus on reactive management of patient crises.
The modern model of heart failure care uses digital technology to support patients at various stages of their heart failure illness, allowing dynamic management of issues as they arise.
Lessons Learned from Remote Monitoring Using Stand-Alone Technologies
The early remote monitoring studies for patients with HF tended to be small, often single centred and of short duration.
Patients were typically recruited at (or shortly after) a heart failure hospitalisation (HFH), and the technologies used were simple and stand-alone. Some of the key studies are listed in more detail in (Table 1).
Such studies are likely to be subject to publication bias (positive studies more likely to be published than neutral or negative studies) and may not have been representative of more routine practice due to the enthusiasm of the single centres (Fig. 2).
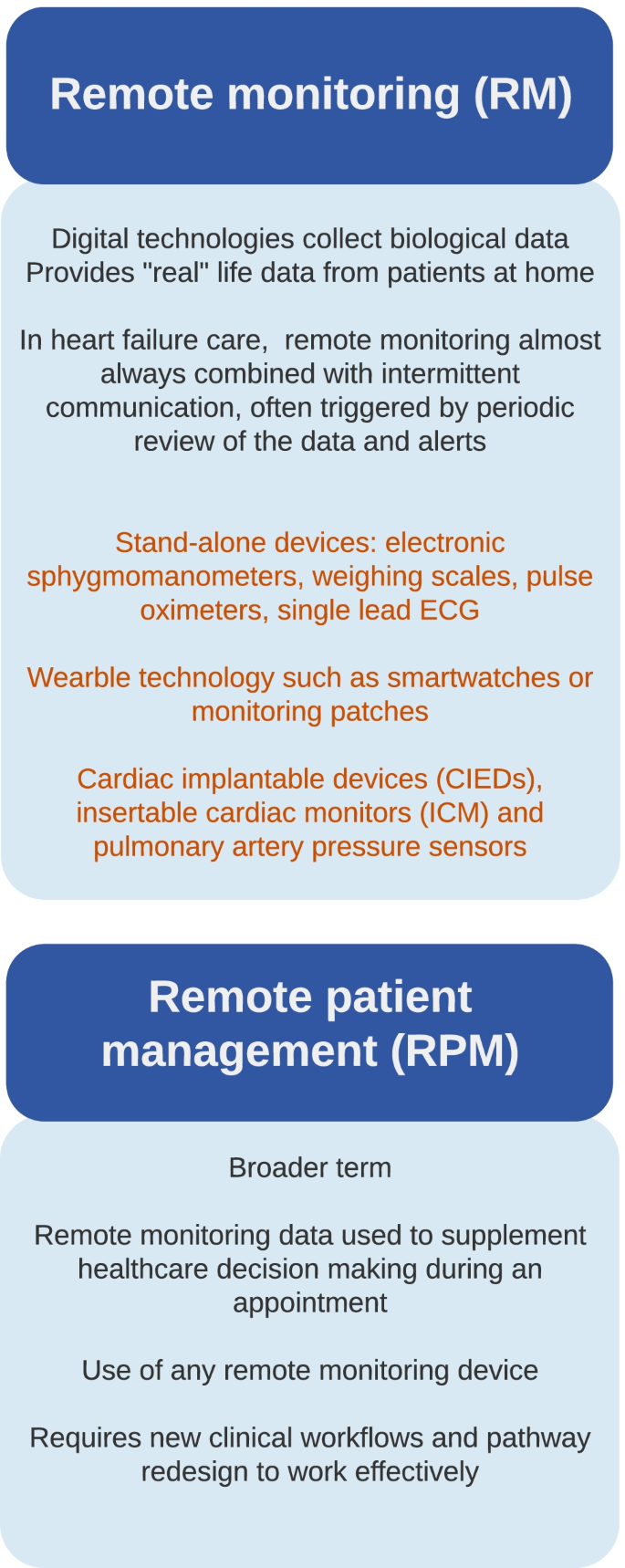
What are remote monitoring and remote patient management?
Meta-analysis of these early small randomised studies suggested a powerful impact on both mortality and hospitalisation compared to usual care [ 13], with a 34% relative risk reduction in mortality ( CI 19–46%, p < 0.0001) and 21% relative risk reduction in heart failure hospitalisation (HFH) ( CI 6–33%, p = 0.008).
How this effect was mediated is unclear but is likely to include improved guideline compliance by HCPs, improved medication and lifestyle compliance by patients, and earlier detection of decompensation with intervention to restabilise the HF syndrome and reduce the need for hospitalisation.
… the results … suggested a powerful impact on both mortality and hospitalisation compared to usual care , with a 34% relative risk reduction in mortality and 21% relative risk reduction in heart failure hospitalisation (HFH)
Except for the encouraging results of two early larger trials [ 7, 19], the next generation of multicentre studies (consequently adequately powered, arguably more likely to be representative of usual practice, and less subject to publication bias) often failed to show a significant difference in “hard” endpoints such as mortality or HFH over 6–20 months of follow-up.
This was despite a variety of patient phenotypes and risk, and a wide range of interventions including devices with embedded reminders and assessment of patient-reported symptoms, structured telephone support with nurse specialists and monitoring of weight, blood pressure, heart rate and ECG [ 8, 9, 20].
TIM-HF2 (Telemedical Interventional Management in patients with Heart Failure) provided the first positive large randomised controlled trial (RCT) in RPM using stand-alone equipment in 710 patients with HF, New York Heart Association (NYHA) class II or III, and a HFH within the preceding 12 months.
TIM-HF2 reported a borderline statistically significant 20% reduction ( p = 0.046) in the primary endpoint of percentage of days lost to unplanned admission or death during 12-month follow-up from 6.64 to 4.88%, with no statistically significant reduction in the secondary endpoint of cardiovascular (CV) mortality ( p = 0.056) [ 12**].
However, it required an intensive and well-resourced approach, with daily review of the monitoring data, ability to stream ECGs and a centralised 24/7 telemonitoring centre in Berlin with close connection with the emergency services, local general practitioners and the patient and their family.
Assessment of the likely cost-effectiveness of this approach, suggested a small cost saving per patient year (€1760) in the German healthcare system [ 21].
TIM-HF2 reported a borderline statistically significant 20% reduction in the primary endpoint of percentage of days lost to unplanned admission or death during 12-month follow-up from 6.64 to 4.88%…
However, it required an intensive and well-resourced approach, …
… the likely cost-effectiveness of this approach, suggested a small cost saving per patient year (€1760) in the German healthcare system
The neutral results from several other large RCTs, and the selected nature of the population within TIM-HF2, led to the most recent European Society of Cardiology (ESC) guidelines to be lukewarm about its recommendation for routine telemonitoring of patient with HF with stand-alone equipment (class 2 level B — “may be considered”). [ 22].
Similarly, weak recommendations have been issued by the American, Canadian and Australian HF societies [ 23, 24, 25].
… the most recent European Society of Cardiology (ESC) guidelines … are found … to be lukewarmabout its recommendation for routine telemonitoring of patient with HF with stand-alone equipment …
Similarly, weak recommendations have been issued by the American, Canadian and Australian HF societies
Rehabilitation and training programmes in HF have used a combination of supervised and unsupervised sessions in hospital and at home.
TELEREH-HF (The Telerehabilation in Heart failure patients) RCT randomised 850 patients up to 6 months after a HFH with NYHA I-III symptoms and reduced ejection fraction [ 17*].
A total of 425 patients received a 9-week hybrid comprehensive telerehabilitation (HCTR) programme encompassing RPM and individualised tele-rehabilitation.
This hybrid approach did not extend the percentage of days alive and out of hospital at extended follow-up: 91.9 (± 19.3) HCTR group vs 92.8 days in the usual care group (± 18.3)( p = 0.74).
However, several physical rehabilitation studies have replicated the other findings of TELEREH-HF, with significant but short-term improvement in symptoms, physical performance, functional capacity and depressive symptoms [ 16, 18, 26, 27] without translating into reductions in mortality or HFH risk [ 15, 17*].
It is likely that cardiac rehabilitation and physical fitness need to be maintained in order to gain long-term benefits [ 28] and may be dependent on improving patient’s capacity for self-management [ 17 *].
Ongoing support by digital technology and remote patient management may facilitate these objectives.
Rehabilitation and training programmes in HF have used a combination of supervised and unsupervised sessions in hospital and at home.
It is likely that cardiac rehabilitation and physical fitness need to be maintained in order to gain long-term benefits [ 28] and may be dependent on improving patient’s capacity for self-management [ 17 *].
Ongoing support by digital technology and remote patient management may facilitate these objectives.
Lessons Learned from Remote Monitoring and Remote Patient Management Using Implantable Devices
- Cardiac Implantable Electronic Devices (CIEDs)
- Remote haemodynamic monitoring
- Wearables
- Technologies in Development
Cardiac Implantable Electronic Devices (CIEDs)
CIEDs record multiple physiological variables — such as heart rate, heart rate variability, episodes of arrhythmia including atrial fibrillation or fast ventricular rhythms, transthoracic impedance, patient activity, and in some systems sleep apnoea and the intensity of heart sounds. Many of these variables are associated with the risk of HF decompensation [ 29, 30].
Initial studies (detailed in Table 2) likely placed too much weight on one variable leading to too many false positives. In the DOT-HF (Diagnostic Outcome Trial in Heart Failure) randomised study, an audible alarm was triggered within the device if a threshold of a decreasing trend in transthoracic impedance (reflection of increasing lung water and left ventricular filling pressure) was crossed. This triggered a 79% increase in HF hospitalisation, and the study was stopped early due to this [ 31]. The human factors triggered by an audible alarm sounding within the device were likely part of the problem: it is difficult for the patient, the family, and the emergency room physicians to ignore an alarm. Many of the admissions were short and with low mortality — suggesting that HF had not truly decompensated, and the admission was often unnecessary.
In the Optilink-HF Study (Optimization of Heart Failure Management using OptiVol™ Fluid Status Monitoring and CareLink™) in just over 1000 patients followed up for an average of 23 months, few actions were taken in response to “alerts” on changes in transthoracic impedance sent by SMS to the responsible physicians, and when action was taken, it was often delayed [ 42]. There is little point in remotely monitoring a patient if the data collected are not rapidly integrated into the decision-making processes.
The IN-TIME (Implant-based Multiparameter Telemonitoring of Patients with Heart Failure) study [ 29] evaluated automatic daily data transmission of multiparametric device data to a single call centre vs. those receiving conventional follow-up through 12 months after ICD or CRT-D implantation in 716 patients enrolled at 36 centres in Australia, Europe and Israel [ 43]. The odds of the primary endpoint of the composite “Packer” clinical score for HF, (comprising all-cause death, overnight HFH, change in NYHA class, and change in patient global self-assessment) worsening in the intervention group was 0.63 (95% CI 0.43–0.90) compared with the control group. A reduction in a secondary endpoint of all-cause mortality was also reported. The authors interpreted their findings as most likely due to the centralized daily review of all monitored parameters, combined with the protocolised and timely actions that were taken in response to the data [ 29]. A pooled analysis of remote monitoring of CIEDs using one manufacturer’s technology (including IN-TIME) reported that active remote management was associated with a 36% reduction in HFH ( p = 0.007) and a borderline significant reduction in all-cause (but not CV) mortality [ 44].
In the larger and longer duration REM-HF (REmote Management of Heart Failure using implantable electronic devices) study at nine large UK hospitals, all the remotely collected data from a CIED was reviewed weekly by a team experienced in HF and remote monitoring [ 35]. They had the time to focus on the remote monitoring processes and worked to a standardised protocol. Despite multiple actions being taken by the monitoring teams in response to the data review of the 1650 patients followed up for a mean of 2.8 years, there was no significant change in either HFH or CV mortality. This study illustrates that without prespecified standard operating procedures, it is not straightforward to translate complex multiparametric monitoring information into “actionable” care strategies to improve clinical outcomes.
The role of insertable cardiac monitors (ICMs) in HF care has been limited currently to the diagnosis of arrhythmia such as sub-clinical atrial fibrillation [ 46]. ALLEVIATE-HF (Algorithm Using LINQ Sensors for Evaluation And Treatment of Heart Failure: NCT04452149), due to report in 2024, will randomise up to 700 patients to an ICM-based risk stratification algorithm (plus a medicines management plan) or usual management. The endpoint is a hierarchical composite of cardiovascular death, HF events, change in Kansas City Cardiomyopathy Questionnaire and change in 6-min walk test distance.
Remote haemodynamic monitoring
The pivotal American CHAMPION trial randomised patients with NYHA class III HF across a range of ejection fraction and reported a 30% reduction in HF hospitalisation risk at 6 months [ 50]. This study, along with other post-marketing randomised and observational studies in the USA and Europe [ 47*, 48, 53, 54], has suggested robust evidence of benefit when used in specialist centres.
More recently, two European studies have shown the likely added benefit in NYHA class III patients in routine care within healthcare systems outside the USA: MEMS-HF (CardioMEMS European Monitoring Study for Heart Failure) in Germany [ 47*] and COAST (CardioMEMS HF System Post-Market Study) in the UK [ 48], with a 62% and 82% reduction in annualised HF hospitalisation rates, respectively. Such data have facilitated positive reimbursement decision making outside the USA, including most recently in England by the National Institute for Health and Care Excellence (NICE) [ 55]. In Germany, health authorities are awaiting the results of PASSPORT-HF (Pulmonary Artery Sensor System Pressure Monitoring to Improve Heart Failure Outcomes [ 56]), a randomised study which compares the efficacy of standard HCP-coordinated HF care (“basic care”) plus PAP-guided management with basic care alone, before a final reimbursement decision is made.
Broadening of the indication for remote PAP monitoring using CardioMEMS™ to less symptomatic patients (NYHA class II) was the purpose of GUIDE-HF (Haemodynamic-guided management of heart failure) [ 52]. Complicated by the COVID-19 pandemic, with huge shifts in patient care patterns during “lockdowns”, the study failed to reach statistical significance overall. A pre-specified pre-COVID analysis (using the majority of data in the study, prior to the first USA COVID-19-related lockdown) suggested a strong evidence of benefit across this broader range of patients (24% reduction in HF events over 12 months, p = 0.014). The FDA has just approved the expansion of the use of CardioMEMS to include patients with NYHA class II HF, provided they have experienced a recent HFH or have an elevated plasma natriuretic peptide concentration [ 57].
Ongoing studies may expand the choice of location of invasive monitoring device beyond PAP sensors, allowing a more personalised approach related to the individual’s physiology. Implant sites currently under investigation in first-in-human safety trials, include the inferior vena cava (FUTURE-HF) and the left atrium (VECTOR-HF). Placed in the inter-atrial septum, preliminary results from the left atrial pressure sensor show it is likely to be safe, the readings show a strong correlation with invasive PAP measurements and there is a signal of improvement in NYHA class [ 58].
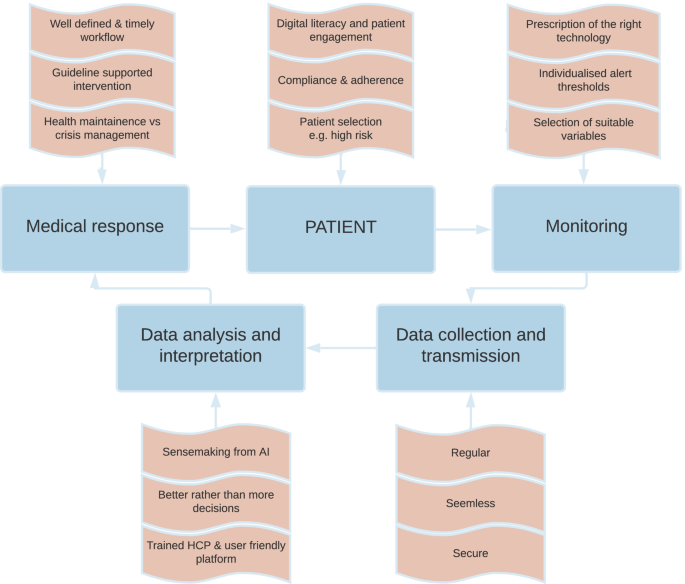
Key elements to consider for successful remote patient management. Modified with permission from Angermann C, 2019 [ 59]. AI, artificial intelligence; HCP, healthcare professional
Wearables (Table 4)
Wearable medical devices (“wearables”) can provide a variety of data from sensors that typically can be worn on the wrist, clipped to clothing or stuck to the skin [ 65, 66 **]. The most studied are “smart” watches, activity monitors and monitoring patches.
Smartwatches and activity monitors typically combine accelerometers, which track movement, with photoplethysmography (PPG), an optical sensor able to monitor heart rates. PPG traces can also be used to assess cardiac rhythm. The Apple™ Heart study used PPG with an “irregular pulse algorithm” to screen patients for atrial fibrillation (AF); 34% of patients with a positive notification subsequently had AF diagnosed on ECG patch testing [ 62]. The accuracy of PPG is hindered by a high dropout rate, changes in position, changes in exercise and rapid changes in heart rate [ 67, 68, 69], and that it does not produce an ECG [ 70]. Despite this, the early results from the Fitbit Heart Study add to the Apple™ Heart study showing the potential utility of wrist-worn wearables in screening of asymptomatic individuals, with likely higher relevance for those at higher risk of AF such as patients with heart failure [ 60], and those at risk of development of the heart failure syndrome due to AF [ 71].
Wearable patch technology is typically placed on the chest wall and can monitor several additional variables including movement, temperature and respiratory rate for a period of days to weeks. This technology greatly increases the diagnostic yield for AF [ 63] but also provides data for multiparametric scores similar to those used with remote monitoring of CIEDs in HF.
LINK-HF [ 64**] (Multisensor Non-invasive Remote Monitoring for Prediction of Heart Failure Exacerbation) studied the VitalConnect™ disposable patch sensor (7-day battery life) with a re-usable sensor electronics module. One module can provide months’ of continuous monitoring. In patients recently discharged after a HFH, the technology was able to identify the risk of further HFH with greater than 76% sensitivity and an 85% specificity in a retrospective analysis — similar to the performance of Medtronic’s Heart Failure Risk Score (HFRS™) and Boston Scientific’s Heartlogic™ algorithm in their development and validation studies in CIEDs [ 33, 37]. Such patch technology may not just be beneficial in monitoring patients at home but also may allow real-time monitoring in hospital and other care settings, although further validation is required [ 73].
Technologies in Development (Table 5)
Examples of novel technologies under investigation to improve RPM in HF include: ReDS (remote dielectric sensor from Sensible Medical), SimpleSense™ (Nanowear), µCor™ (Zoll®) and HearO™ (Cordio Medical).
Examples of novel technologies under investigation to improve RPM in HF include: ReDS (remote dielectric sensor from Sensible Medical), SimpleSense™ (Nanowear), µCor™ (Zoll®) and HearO™ (Cordio Medical).
ReDS uses an electromagnetic based technology developed by the military to provide an instantaneous estimation of lung fluid content. Using ReDS to guide management in recently discharged patients with HF demonstrated a halving of the rate of HFH over 6 months in a non-randomised study [ 74]. The ReDS-SAFE HF trial is currently randomising up to 240 patients admitted for HF at one US centre, to ReDS-guided discharge or usual care, with a primary composite endpoint of unplanned visit for HF or all-cause mortality ( NCT04305717).
SimpleSENSE™ is an FDA-cleared wearable undergarment that monitors several vital signs such as heart rate, heart sounds, respiratory rate, lung volume and physical activity and is connected to a machine-learning platform. Results are awaited from a cohort study developing and validating a multi-parametric algorithm to detect HF decompensation.
µCor is an ECG patch and HF management system that uses radiofrequency technology to measure multiple parameters including thoracic fluid index. A multicentre trial aims to correlate this to the risk of HF events ( NCT03476187).
Voice detection algorithms allow the HearO™ mobile phone application to assess fluid status and highlight the difference between pre- and post-dialysis states [ 84], and through fluid optimisation during a HFH [ 81].
Factors Affecting the Development and Use of Digital Tools in HF Care
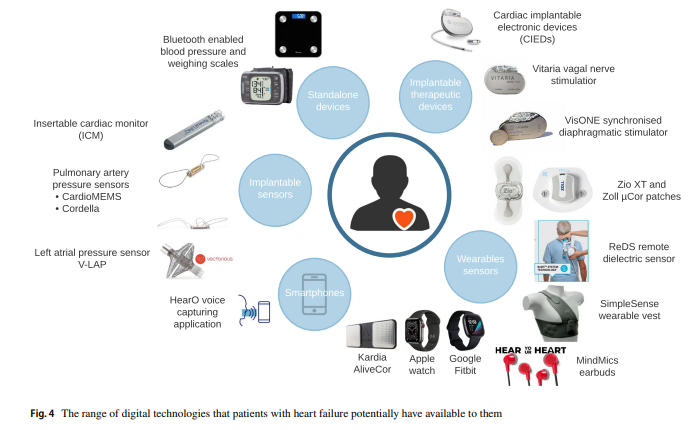
There are an increasing range of digital technologies available to support remote patient management in HF (and other diseases) (Fig. 4) but several factors are pivotal to their optimal development, maintenance, and longer term use.
We have expanded on these issues in our commentary in this edition of the journal, entitled The Digital Future of Heart Failure Care.
They include issues around the evaluation and regulation of technology, co-design and co-implementation, data security and access, machine learning in support of decision-making and litigation risk.
Key to success is a better understanding of the support needs and capabilities of patients living with HF (and their healthcare advisors) including their digital and health literacy and degree of activation.
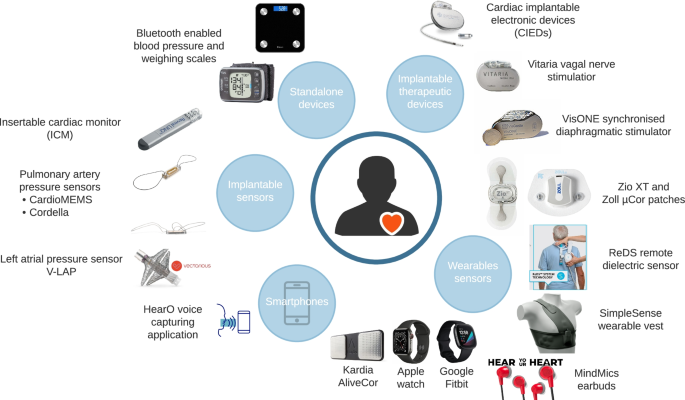
The range of digital technologies that patients with heart failure potentially have available to them
Right Technology, Right patient, Right time: a Vision of the Future
The traditional model of HF care with periodic clinic review, using only data collected at that time by the healthcare team using “their” technologies, is likely to be replaced (or at least supplemented) by a more patient-centric approach.
Collecting data remotely provides “real” life data — which represent more than 99% of the time when patients are in their own environment — to be used in shared decision-making.
The traditional model of HF care with periodic clinic review, using only data collected at that time by the healthcare team using “their” technologies, is likely to be replaced (or at least supplemented) by a more patient-centric approach
Collecting data remotely provides “real” life data — which represent more than 99% of the time when patients are in their own environment — to be used in shared decision-making.
Shared decision-making requires a good working relationship between patient and HCP, as well as a patient who is adequately informed, educated and (therefore) motivated to make changes based on remote monitoring data.
Access to HCPs and systems will still be needed and must be available flexibly and at potentially short notice, but much of the routine processes of care can be supported by technology and RPM, freeing up time and bandwidth for members of the healthcare team to deal with the more complex, or nuanced, situations where human-to-human interaction adds more value.
In practice, digital remote technologies will support the key activities within the care pathway — ensuring rapid and accurate diagnosis, risk stratification and prognostication, therapeutic decision-making and tailored support including education and care.
Active shared decision-making between clinician and patient will decide which technology can best be used to achieve the shared goals, whether it is initial education and support to self-care, identification when another therapy may be beneficial, or helping the patient maintain stability with optimised quality of life at home, without the need to engage with the “official” healthcare system by attending clinic or being hospitalised.
Technology should provide closed-loop interactions with patients, offering advice on fluid intake, diuretic regime, exercise, necessity for blood tests and when to contact an HCP.
When patients require input from an HCP they deserve a tailored and responsive interaction based on multiple relevant data points and sources, with decision and sensemaking supported by digital tools (and likely artificial intelligence).
Clinical deterioration will be predicted and identified early using remote monitoring and stabilisation facilitated by appropriate escalation of therapy.
Admission to hospital will, of course, remain necessary for some patients, but early discharge will be supported with virtual wards (“hospital-at-home”) with monitoring pathways and rehabilitation facilitated remotely.
We highlight the differences between the traditional model of care and this more modern, digitally enabled approach to HF care in Fig. 1.
Conclusion
Digital technologies are already deeply embedded within all aspects of society, including health and healthcare.
HF care already relies on many of them, but the clinical pathways and treatment algorithms to successfully integrate digital technologies and decision support into the healthcare system are in their infancy.
Ultimately, digital technologies will become part of the “new normal”, being selected for use when they make sense and help patients and their HCPs achieve shared goals.
Digital technologies are already deeply embedded within all aspects of society, including health and healthcare.
HF care already relies on many of them, but the clinical pathways and treatment algorithms to successfully integrate digital technologies and decision support into the healthcare system are in their infancy.
Ultimately, digital technologies will become part of the “new normal”, …
Due consideration must be paid to ensuring the evidence base is robust, that data flows and human factors are considered, and that the digital technologies are co-designed and implemented to ensure a better outcome and experience of care.
Data should not be collected for its own sake — it must support better decision-making and more efficient care.
Authors & affiliations
Royal Brompton Hospital (Guy’s & St Thomas’ NHS Foundation Trust), Sydney Street, London, SW3 6NP, UK
K. C. C. McBeath & M. R. Cowie
Comprehensive Heart Failure Centre, University and University Hospital Würzburg, Würzburg, Germany
C. E. Angermann
School of Cardiovascular Medicine, Faculty of Medicine & Lifesciences, King’s College London, London, UK
M. R. Cowie
References and additional information
See the original publication
Cite this article
McBeath, K.C.C., Angermann, C.E. & Cowie, M.R. Digital Technologies to Support Better Outcome and Experience of Care in Patients with Heart Failure. Curr Heart Fail Rep (2022). https://doi.org/10.1007/s11897-022-00548-z
About the authors & affiliations
K. C. C. McBeath 1 ·
C. E. Angermann2 ·
M. R. Cowie1,3
1 Royal Brompton Hospital
(Guy’s & St Thomas’ NHS Foundation Trust), Sydney Street,
London SW3 6NP, UK
2 Comprehensive Heart Failure Centre,
University and University Hospital Würzburg,
Würzburg, Germany
3 School of Cardiovascular Medicine,
Faculty of Medicine & Lifesciences,
King’s College London, London, UK
Cite this article
McBeath, K.C.C., Angermann, C.E. & Cowie, M.R. Digital Technologies to Support Better Outcome and Experience of Care in Patients with Heart Failure. Curr Heart Fail Rep (2022). https://doi.org/10.1007/s11897-022-00548-z
Originally published at https://link.springer.com on April 29, 2022.







