




Site editor:
Joaquim Cardoso MSc.
Health Transformation — institute for research and strategy
October 6, 2022
This is an excerpt of the article “Mortality Rates for Medicare Advantage Are Actually Significantly Lower and Better, with Fewer Deaths ”, with the title above, focusing on the topic in question.
Intergroup Institute
George C. Halvorson
September 30, 2022
Some of the Best Care in America is in Medicare Advantage Special Needs Plans
The people who continue to accuse Medicare Advantage in public settings and even in some policy settings of exaggerating the health care needs of their patients in order to somehow distort plan diagnosis codes should be ashamed of themselves for distorting the truth so significantly at so many levels and they should look directly at the actual programs that they clearly do not say they see today and they should honestly acknowledge what they see there today.
People with some of the highest health care needs in America are in those plans and they are getting great care and giving those programs extremely high levels of satisfaction as members.
Our biggest policy and one of our top functional concerns as a nation today should be that only half of the people who could qualify for those programs are currently enrolled in the plans, …
…and that is very bad for the country and those patients because the people who are not in the plans are much more likely to have their leg amputated and much more likely to go blind.
We have good and credible context information about the overall managed care programs from multiple sources, and we should be using that information to understand what the plans are doing.
We do have some very good context information to help us understand what the plans are going.
In addition to that set of data from multiple sources, we need to understand the importance of the work done by the Health and Human Services team who carefully took a clear and systematic look at all of the variation of managed care purchased today as a package by the government — and that data gives us solid grounding to look at all of the other data from a highly credible perspective that underscores the importance and credibility of that work.
We are extremely fortunate that we have that great new report from the government that we can use to putting those important issues into perspective at a time when there continues to be debate from some critics on some extremely inaccurate issues relative to the performance of the plans.
A lead chart from that important and grounding new report is at the very top of this discussion piece. [see reproduction below]
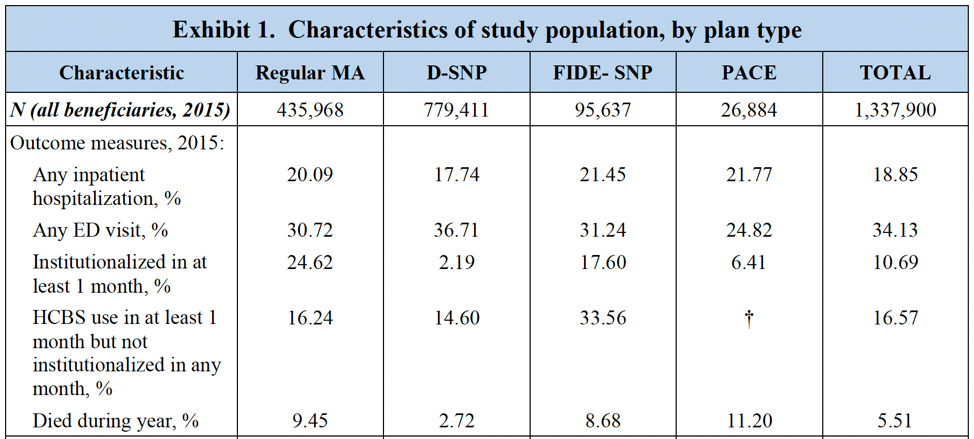
Health and Human Services just did an excellent overview of the four Medicare Advantage types of plans and they achieved some important new data point about the current performance of the plans that included, for the first time ever, showing us the mortality rates from each of the programs.
This official “final” outcomes report from The U.S. Department of Health and Human Services is actually called “Comparing Outcomes for Dual Eligible Beneficiaries in Integrated Care,” and it does exactly that.
That report gives us an extremely robust, well researched, extensive, inclusive, and solid look at the actual performance of the four managed care plans used now by the federal government and that study is worth reading by anyone who wants to get a sense of what those programs are, what they do, and how well they do it.
That report shows that the mortality rate for the two most tightly managed Medicare Advantage programs that reach out to people with special needs is extremely low and that information about the low mortality of those members ought to be extremely encouraging and informative for anyone looking at the future of Medicare funding and at the trajectory and the performance of the Medicare Advantage plans.
… the mortality rate for the two most tightly managed Medicare Advantage programs that reach out to people with special needs is extremely low and …
… that information about the low mortality of those members ought to be extremely encouraging and informative for anyone looking at the future of Medicare funding and at the trajectory and the performance of the Medicare Advantage plans.
The Medicare Advantage plans have had some open, consistent and extremely persistent critics who have made disparaging and too often inaccurate statements and who have created some very wrong and misleading reports about plan performance, and so it was a very good thing to have the new federal Office of Behavioral Health, Disability, and Aging Policy doing this study and then releasing the data to everyone with interest in those issues who wants to have a sense of what is true for the performance of the plans.
They Counted Actual Deaths in Each Program to Get the Mortality Rates
They didn’t just do actuarial approximations or statistical estimates or expert opinion judgement calls to get a general sense of the death rates when they did that report.
They actually used direct Medicare data for each program and they counted the actual deaths for each group.
We have better data than we have ever had on major components of the population being served by the Medicare managed care plans and that data collection and reporting extends to showing differences in the mortality rates of each of the four categories of managed care patients.
The chart shows that the mortality rate for the programs ranges from 2.72 at the low end to 11.2 percent …
… at the high end for the specific actual managed care and Medicare Advantage plans that the government currently uses.
The highest number on that mortality chart is the 11.2 percent that happens in the PACE care system and is not a formal Medicare Advantage plan.
The PACE funding approach and program of community and neighborhood linked care teams strongly resembles Medicare Advantage at multiple levels and it was included in the report because it is the other way that Medicare pre-pays for care.
Care in the PACE program is an excellent, experienced, historically significant patient-focused systems-based and highly neighborhood-based care delivery approach that was targeted at “Frail” seniors and actually preceded Medicare Advantage as a program.
It was set up to avoid hospital care for the people who organized in their communities.
It has some similar patterns of care and it continues to provide neighborhood linked team family- and friend-linked care that is highly superior at every level to the fee-for-service Medicare delivered multiple levels in every PACE setting.
The government included the PACE patients in the study to be inclusive.
Because they are a Medicare managed care program it’s good to know how those patients are doing with their patterns of care.
The data shows that they are doing some good work on their care and it is interesting to see some of the variations in care that can result when frail in home patients are your original focus.
We should definitely have the people who did this particular study do follow-up studies …
… to take advantage of the expanded data flow from the encounter reporting for the Medicare Advantage plans and this should not be a final report — but this information in this report is extremely well done and well timed as we look at the future of Medicare financing and the report gives us a sense of security that the four basic programs are on some good trajectories.
Survival rates were an unexpected new addition to the reporting agenda and to the reporting data flow, …
… and we now know that they make extremely good sense as an addition factor for our data flow about care and they tell us some important information about the plans at an important time to have that information.
Survival rates are a useful way of determining at a very basic level whether or not we are receiving good care because surviving is a good outcome for care and it turns out that they can have some variations that can guide us in good directions.
Survival rates are a useful way of determining at a very basic level whether or not we are receiving good care because surviving is a good outcome for care and it turns out that they can have some variations that can guide us in good directions.
They are particularly relevant here because we know from multiple sources and data flows that fee-for-service Medicare far too often delivers bad care and sometimes clearly dangerous care.
We know that fee-for-service Medicare has the highest rates of blindness for our older population in the world …
… and we know that fee-for-service Medicare has the highest rates of amputations for our older population — with $6 billion worth of amputations being done each year for our older Americans — and we haven’t had a good mechanism for creating a context around those issues that explains how Medicare Advantage has very different approaches to those areas of care and to measure the final impact of that care.
… fee-for-service Medicare has the highest rates of blindness for our older population in the world and …
… fee-for-service Medicare has the highest rates of amputations for our older population — with $6 billion worth of amputations being done each year for our older Americans
We also need everyone in America to realize that those bad outcomes for fee for service Medicare beneficiaries do not need to happen.
The policy people too often look at those bad outcomes and regard them as being somehow inevitable and a normal consequence of care for Medicare patients and then completely leave those bad and damaging outcomes out of too many high-level policy discussions about the traditional Medicare program.
The policy people too often look at those bad outcomes and regard them as being somehow inevitable and a normal
That is shortsighted and almost unethical thinking for us to not focus attention on those failures in a clear, direct, visible, and constructive way …
… because they damage so many Americans every day and the damage has a permanent and unnecessary impact on too many lives.
We know from extensive science and extensive care experience that diabetic blindness can be massively reduced and prevented for most people with the right treatment.
We know now beyond any doubt that the right treatment is much more likely to happen in our Medicare Advantage settings and it is extremely rare in far too many of our fee-for-service Medicare settings.
… beyond any doubt that the right treatment is much more likely to happen in our Medicare Advantage settings and it is extremely rare in far too many of our fee-for-service Medicare settings.
We also know that poor people with diabetes are much more likely to lose limbs in this country …
… because fee-for-service Medicare has no programs to change that terrible pattern of care and we know that only Medicare Advantage patients regularly get the right treatments and prevention services in large numbers of settings.
We also know that poor people with diabetes are much more likely to lose limbs in this country because fee-for-service Medicare has no programs to change that terrible pattern of care and …
… only Medicare Advantage patients regularly get the right treatments and prevention services in large numbers of settings.
Originally published at https://www.intergroupinstitute.org on September 30, 2022.







