




Harvard Business Review
by Nikhil R. Sahni, Robert S. Huckman, Anuraag Chigurupati, David M. Cutler
November-December 2017
IN BRIEF
The Problem
- In recent years, health care organizations and the U.S. government have invested tens of billions of dollars in information technology.
- So far they have little to show for it: The impact on the cost and quality of clinical care has been modest, and productivity growth in the sector continues to lag that of other industries.
The Root Cause
- The priorities of most providers have been replacing paper records with electronic ones, improving billing to maximize reimbursements, and monitoring existing clinical processes.
The Solution
Use IT to transform clinical care. This entails
- emphasizing the improvement of care over cost cutting,
- making data collection easier and better,
- turning the data into actionable information for clinicians, and
- forging new operating and business models.
Structure of the publication
- Introduction
- Improving Quality
- Making Data Collection Easier and Better
- Turning Data into Actionable Information
- Forging New Operating and Business Models
- Conclusion
In the mid-1990s, everyone knew that health care organizations across the United States were plagued by wasteful spending.
The question for Intermountain Healthcare, which serves residents of Utah and Idaho, was where to start looking for savings internally.
Data analyses quickly identified the most promising targets:
- 104 of the 1,440 clinical conditions that Intermountain treated accounted for 95% of the care it provided,
- and two services-newborn delivery and treatment of ischemic heart disease-accounted for 21% of its work.
Quality-improvement teams focused first on those two services.
Armed with a sophisticated electronic health record (EHR) system and a separate information technology system that detailed the costs of activities, the teams used evidence-based guidelines and the experience of Intermountain’s physicians to redesign clinical workflows.
The top executives, the board of trustees, physicians, and nurses all worked together to support the drive to improve care.
Today more than 60 services have been revamped, and Intermountain is recognized as a national leader in quality improvement and cost management.
None of it would have been possible without its IT systems.
This example is impressive. Unfortunately, it is still a rarity.
The more common story in health care is one of large IT investments but little to show for them.
Spurred by examples like Intermountain, the U.S. government’s Centers for Medicare and Medicaid Services spent $37 billion just in incentive payments for health care IT from 2011 to May 2017.
By 2016, more than 50% of office-based physicians and over 80% of hospitals had installed a “basic” EHR system-one that meets minimum standards set forth by the Office of the National Coordinator for Health Information Technology.
Yet such systems have had little impact on quality improvement and cost reduction to date.
Indeed, clinicians routinely criticize them, lamenting that they waste their time, are rigid and not user-friendly, and interfere with their patient interactions.
Many health care organizations are suffering more pain than gain as they struggle to integrate new IT systems into their operations.
For example, in January 2017, MD Anderson Cancer Center announced that it would lay off 900 employees, or about 5% of its workforce, largely because of financial losses attributable to a new EHR system.
More broadly, efforts to persuade health care organizations to share information continue to lag, as do efforts to enable different IT systems to communicate with one another, causing data to remain “stuck” within siloed databases.
A central reason the negatives seem to outweigh the positives is the way IT systems are being used.
To date, the priorities of most health care organizations have been replacing paper records with electronic ones and improving billing to maximize reimbursements.
Although revenues have risen as a result, the impact of IT on reducing the costs and improving the quality of clinical care has been modest, limited to facilitating activities such as order entry to help patients get tests and medications quickly and accurately.
Relatively few organizations have taken the important next step of analyzing the wealth of data in their IT systems to understand the effectiveness of the care they deliver.
Put differently, many health care organizations use IT as a tool to monitor current processes and protocols; what only a small number have done is leverage those same IT systems to see if those processes and protocols can be improved -and if so, to act accordingly.
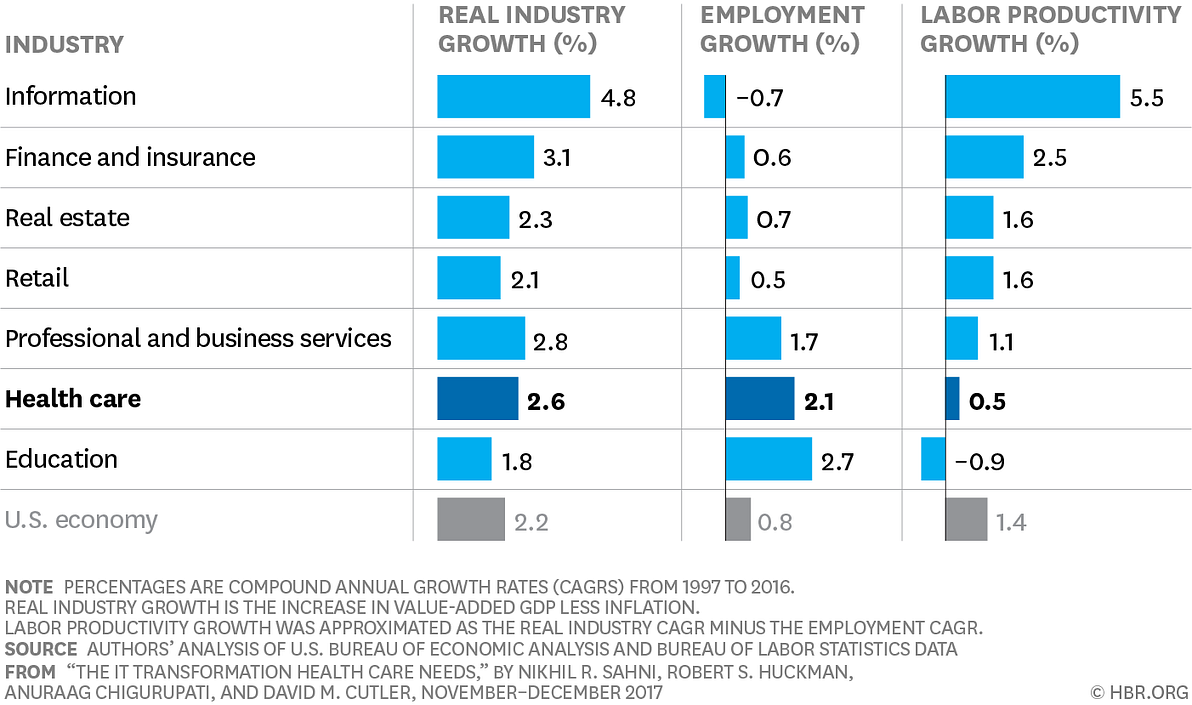
This is a significant reason that productivity growth in health care has been anemic and weaker than that in many other industries.
Some industries use technology better than others, and labor productivity statistics reflect that.
In the case of U.S. health care, the industry has been growing faster than the overall economy, but because the number of health care workers has been rapidly increasing and the use of information technology has lagged, productivity growth has been minimal.
So how can health care organizations realize the promise of their large and growing investments in IT to help lower costs and improve patient outcomes?
While substantial attention has been paid to the potential medical benefits of new technologies such as inexpensive genetic screening, artificial intelligence, and wearable sensors that continuously monitor vital signs, our main focus is on how the organizations that deliver care can get much more out of their recent or planned investments in enterprisewide IT systems.
Our research on the ways health care could apply the experiences of other industries suggests that instead of viewing IT as a transactional tool …
… for billing, monitoring, and error checking, organizations should embrace it as an instrument to help transform the way they deliver medical care.
This will entail prioritizing quality improvement over cost cutting, making data collection easier and better, turning the data into actionable information for clinicians, and forging new operating and business models.
We have found that while numerous health care organizations are moving in this direction, the majority are not making the holistic changes needed for transformation.
Improving Quality
Historically, the adoption and management of health care IT has been left to an organization’s chief information officer and other technical personnel. This is a mistake.
A number of organizations-including Boston Medical Center, Geisinger Health System in Pennsylvania, Intermountain, Mayo Clinic, and New York University (NYU) Langone Health-have shown that health care IT is effective only when all members of an organization work to unlock its potential.
(Full disclosure: One of us, Robert Huckman, has taught in executive education programs for two organizations related to this article-Intermountain Healthcare and Brigham and Women’s Hospital, which is owned by the same parent company as Massachusetts General Hospital.)
Two key constituencies outside of technical personnel-senior leaders and clinicians-must play significant roles.
Leaders are crucial because they will have to enlist clinicians in the cause by persuading them that the effective use of IT is central to delivering higher quality.
The urgent need to reduce health care costs has led many leaders to become preoccupied with that objective.
The happy reality is that improving clinical work processes can achieve both lower costs and higher quality, and we’ll discuss later what it takes to use IT systems to do this.
The pledge to improve quality should be more than words; it must be translated into visible practices.
Geisinger, for one, has done just that. It has made its IT system part of a broad strategy to establish a surgical “warranty”: If complications arise within 90 days of a surgical procedure, the patient bears no additional cost to have the problem addressed.
Starting with coronary artery bypass grafting (CABG), a team of clinicians developed a five-stage protocol that begins at the time of diagnosis and extends through the warranty period.
The team initially identified 40 evidence-based guidelines that, according to a case study conducted by the Commonwealth Fund, were then embedded in the EHR system “through templates, order sets, and reminders,” driving up adherence from 59% to 100%.
Furthermore, the integrated IT system improved communication among various clinical personnel (including physicians and advanced-practice nurses) to coordinate care for the patient.
The results were significant:
- Postoperative mortality fell by two-thirds, post-acute-care spending decreased by nearly 50%, and
- the overall profitability of cardiac surgical services actually improved.
Thanks to the success of the CABG program, the model was expanded to 14 other clinical conditions as well as to primary care, with a focus on the chronically ill.
NYU Langone Health has also backed up its words about improvement with action.
When Dr. Robert Grossman became the center’s CEO and the dean of NYU School of Medicine in 2007, his first major initiative was to merge the school’s disparate information systems into a single data warehouse for both the hospital and the medical school.
He stressed that the reason was to evaluate the system’s quality performance against external benchmarks and to support changes in administrative and clinical workflows.
The resulting information increased the willingness of department chairs and administrators to challenge norms and to design and implement improvements.
For example, the need to establish data fields in the IT system forced discussions about the definition of “excellence” and the best ways to assess the impact of frontline staff.
In 2016, NYU Langone received multiple national quality awards and was ranked by U.S. News & World Report among the top 10 hospitals in the United States, alongside the likes of Mayo Clinic, Cleveland Clinic, and Massachusetts General Hospital.
The organization’s financial performance was similarly impressive: From 2007 to 2015, patient revenues more than doubled.
NYU Langone now generates more than $220 million in operating profit, with an operating margin above 9%.
Notably, both Geisinger and NYU Langone found that achieving their quality goals did not come at the expense of financial performance. In fact, that also improved.
Making Data Collection Easier and Better
Having high-quality data at the right time is critical to tracking and measuring outcome improvement.
Yet the data collection methods that most health care organizations use are inefficient, administratively burdensome, and likely to produce errors.
It is nearly impossible to speak to a group of clinicians without the conversation quickly turning to the time-consuming task of gathering medical information and entering it into a new IT system.
A time and motion study published in the Annals of Internal Medicine in 2016 found that physicians spend one to two hours each night after their workday mostly on EHR tasks.
This addition to their already heavy workload is contributing to the epidemic of physician burnout in the United States.
And studies show that these problems cause physicians to take shortcuts such as copying and pasting notes and rapidly clicking through alerts, undermining the quality of the data that’s collected.
In response, many organizations now employ medical scribes to enter information into EHR systems on behalf of clinicians.
Yet the awkwardness of having a third party in an examination room-not to mention the added cost-makes the use of medical scribes controversial.
Moreover, patient information that is gathered and entered into the system in this manner is prone to error.
The remedy: Shift data collection from an “event” that takes time and may be performed inaccurately to one that occurs “in the background” as clinicians and patients engage in their natural activities.
The retail industry shows what’s possible.
During the past few decades, retail has experienced two significant shifts with respect to who collects data and how.
One example is checkout. Cashiers used to have to key the price of each item into a cash register. The introduction of bar code scanners sharply reduced the amount of time cashiers spent on that task, decreased data-entry mistakes, and greatly improved inventory management. Next, it became possible for many customers to scan their own items.
Amazon is now taking things one step further by piloting its Amazon Go brick-and-mortar store, which eliminates checkout lines altogether.
Instead, a passive data-collection system relies on computer vision, deep-learning algorithms, and sensors to automatically read what exiting customers have in their shopping baskets.
Other retailers, including Kroger and Apple, are experimenting with analogous models.
In health care, a similar transition has begun but is moving slowly.
One trend is to shift the job of collecting information from clinicians to patients.
For example, after a primary care physician and a patient agree to address a clinical goal such as reducing blood pressure or blood sugar levels, they can enter that goal and the associated treatment plan into one of the health-monitoring apps offered by a number of companies.
Patients then measure and report their activity and clinical information on a regular basis through the app.
In some cases, data collected by the patient at home is automatically shared with his or her clinician.
One example is the Hypertension Digital Medicine (HDM) program developed by Ochsner Health System.
Through smartphone technology, blood pressure readings taken remotely by patients are fed directly into Ochsner’s EHR system, allowing physicians to review data between visits and course-correct a patient’s care plan.
In a controlled trial reported in the American Journal of Medicine, 71% of participants brought their blood pressure down to the normal range within 90 days, compared to only 31% in the control group. The patients using HDM also reported 10% higher satisfaction with their health care.
Ultimately, the goal should be to move to truly passive data collection.
Some pioneers are using passive collection to track operational issues related to workflow and resource utilization.
Mayo Clinic developed a real-time location system (RTLS) that uses radio-frequency identification tags and sensors to track staff, patients, and equipment in its emergency department.
This data allowed the department to better understand how care was delivered, identify operational barriers, and fix workflow issues.
Then the information was used to develop systems for automatically collecting process-quality metrics (such as the time between a patient’s registering at the emergency department’s front desk and being put in a bed and seen by a clinician) and automatically reporting that information to government agencies and regulatory bodies. (See “How RFID Technology Improves Hospital Care.”)
Similarly, Rush University Medical Center in Chicago built a new outpatient practice with RTLS sensors for each room, clinician, patient, and piece of equipment.
The system alerts staff when a patient leaves his or her exam room, eliminating the need for a practice manager to inform cleaning staff that a room needs to be serviced and preventing awkward interruptions of patients who are still dressing after an appointment.
The time saved per patient is relatively small-perhaps just one minute.
But over the course of a day, the total savings allow clinicians to see more patients, thereby improving productivity.
Over time, as passive-data-collection technologies become less costly and as clinicians and patients become more comfortable with them, the benefits will increase.
This will help organizations justify the upfront cost and make it easier to overcome hurdles such as employee concerns about being monitored.
Turning Data into Actionable Information
Persuading clinicians to engage with a new IT system-and making it less burdensome for them to do so-is only half the battle.
Turning the data collected into actionable information is also vital and requires senior leadership’s support.
One of the most critical tasks for a leader is to set expectations for how the system will be structured.
We’re talking not about the technical specifications but about organizational or cultural guidelines for using the data to support daily care-related activities.
A key step is establishing a core data warehouse for the organization and getting clinicians to understand its importance.
In making the case to the staff of NYU Langone, Grossman emphasized the value of having a single source of truth across inpatient facilities, outpatient centers, and the medical school.
In the process of developing the data warehouse, various parties at NYU Langone that were previously protective of their turf and information were forced to work together.
Disputes over which of several data sources were accurate ended, and Grossman persuaded department chairs to start using tools such as data dashboards to assess what was (and was not) working across departments.
Over time, as the benefits of the resulting transparency became apparent, clinical leaders’ initial skepticism about the IT system subsided.
Departments would receive data on quality metrics for peer departments within NYU Langone (the rates of hospital-acquired infection in different parts of the hospital, patients’ length of stay, and so on), and they could then determine whether and how to change their own workflows.
Beyond encouraging the development of the necessary data infrastructure, senior leaders must also help establish a vision for how the collected data will be used to improve productivity.
In many cases, pursuing the vision may involve supporting the creation of entirely new measures of performance.
Sabermetrics, the mathematical analysis of baseball data, offers an example of how new measures-and technologies to collect and analyze the information related to them-can revolutionize an industry.
Developed by statisticians (the most prominent of whom is Bill James), sabermetrics involves measuring aspects of the performance of individual players and calculating their contributions to team outcomes. Initially, gathering the data was tedious.
As sabermetrics pioneers found homes in big-league clubs, however, data warehouses were developed to ease collection and analysis.
Since 2015, high-resolution cameras and Doppler radar have been installed in all stadiums to glean previously hard-to-track information, such as speed and acceleration, to quantify a player’s defensive prowess.
This in turn has led to the creation of entirely new metrics such as “wins above replacement,” which has become the standard, all-inclusive measure of an individual’s value to a team.
Compared to other industries, health care is in a relatively early stage of applying analytics. But the promise is great.
For example, a small but growing number of health care organizations have built sophisticated systems that facilitate a deep understanding of costs and quick illustration of how innovations in providing care can improve both outcomes and costs.
Intermountain was a pioneer in this realm, but others are following suit.
Recently, University of Utah Health created a system with a 200 million-row database that yields information on key operational metrics such as cost per minute in the emergency room.
According to a New York Times article, the organization has used this information to change operational workflows, reducing costs by 0.5% a year over the past few years, whereas other academic medical centers in its market area averaged annual increases of 2.9%.
Another important use of analytics is identifying unnecessary variation in treatment.
A good example is New York-based Crystal Run Healthcare, a physician-owned multispecialty medical group that wanted to standardize treatment for 15 diagnoses that were common among its patients.
As reported in a Health Affairs blog post, the organization first calculated the total annual cost per patient-segmented by professional, laboratory, radiology, and procedure charges-and then examined the cost of care across physicians so that each could see how he or she compared to colleagues on each dimension.
With this information, Crystal Run analyzed the variation, determined its root cause, and instituted some new practices.
Within a year, variation in treating 14 of the 15 diagnoses declined, saving over $4 million. By our estimates, that represented more than 10% of Crystal Run’s medical costs.
IT systems also offer health care organizations an opportunity to use predictive analytics to guide future clinical and operational decision making.
Predictive models in precision medicine are being developed to correlate particular genetic mutations with specific forms of treatment.
Although the use of precision medicine has been most prevalent and publicized in cancer care, it is now being applied in a wider range of specialties.
For example, the GeneSight test can improve the management of depression by using a patient’s genetic information to predict a response to each of 26 available psychotropic medications.
Health care organizations can also use predictive analytics to make better operational decisions about allocating resources and setting priorities for clinical innovations.
For instance, Massachusetts General Hospital identified cohorts of high-risk patients and developed a proactive care-management program around this population.
- Hospitalizations of such patients dropped by 20%,
- their emergency-department visits declined by 13%, and
- the annual cost of caring for them fell by 7% over a three-year period.
- Mortality, physician satisfaction, and patient experience also improved.
Similarly, Boston Medical Center (BMC) used its health care IT system to predict when its inpatient units could expect a surge in demand.
The tool estimated the number of discharges needed in 24 hours by incorporating current demand in the emergency department, demand predicted for the following day, surgical cases requiring an inpatient bed the following day, and current bed and physician capacity.
In its first year of implementation, the number of “code yellows”-warnings that occur when there is not enough capacity to absorb expected demand-decreased by nearly 50%.
Predictive models have the potential to become increasingly useful, and that might happen soon.
As natural-language processing and machine learning expand, more insights will surface from the wealth of data available in health care IT systems. (See “How Machine Learning Is Helping Us Predict Heart Disease and Diabetes.”)
Forging New Operating and Business Models
In its 2012 report Best Care at Lower Cost: The Path to Continuously Learning Health Care in America, the Institute of Medicine (IOM) highlighted ways to leverage IT to improve the U.S. health care system.
Five years later, the first recommendation-the creation of digital infrastructure to capture clinical, care process, and financial data-is approaching completion.
The IOM’s second recommendation was to make data available to clinicians when they are deciding how to treat patients. This is being done sporadically.
For example, Intermountain recently partnered with Cerner to create a flexible clinical-support system containing protocols that can be easily updated with the latest knowledge.
To facilitate the right inputs, Intermountain’s clinical-development teams continuously monitor the various specialties’ evidence-based practice guidelines and are translating them into IT tools that assist medical personnel as they work.
Besides acquiring the necessary hardware and software, leaders must make complementary changes in their operating and business models to generate and capture value.
Of primary importance is investment in dedicated information-technology and analytics staff-individuals tasked with managing the IT system or analyzing the data it contains.
After installing its new EHR system, BMC expanded its permanent IT staff by more than 40% to manage and further develop its IT infrastructure.
It also expanded its strategy team to seven FTEs who extract information from the vast troves of data.
This group investigates and coordinates responses to key operational challenges, including managing inpatient bed capacity and reducing readmission rates.
After installing its new EHR system, BMC expanded its permanent IT staff by more than 40% to manage and further develop its IT infrastructure.
It also expanded its strategy team to seven FTEs who extract information from the vast troves of data.
The savings for BMC amount to millions of dollars, far exceeding the cost of the FTEs.
Specialized teams of clinical personnel are also needed to translate the insights from the analyses into better ways of providing care.
For example, BMC’s efforts to reduce code yellows involved the redesign of a bed-control team-a group of frontline staff and managers who track current inpatient demand and assess potential demand for the next day.
The team members originally entered data into a simple spreadsheet; now they trigger a set of actions-such as adding ancillary support staff, alerting medical units, and opening additional beds-according to data and analysis from BMC’s IT systems.
The data that robust IT systems can provide also plays a crucial role in securing clinicians’ support for workflow changes.
For example, when Grossman first shared a dashboard with NYU Langone’s clinical leaders, he heard complaints about the quality and consistency of data.
Instead of letting that derail the project, he put the onus on the leaders, telling them to either work with IT to fix the data or accept the results. At the end of this process, the data was considered the single source of truth throughout the medical center and the basis for future analytical efforts.
This made it easier for the organization to track metrics consistently.
The dashboard now helps clinical leaders work with frontline staff to implement interventions to improve care delivery, track what is and isn’t working, persuade resistant clinicians to adopt new protocols, and reduce variation in treatment practices.
Beyond these workforce and operational changes, health care organizations will have to rethink their business models in order to capture the full value of their IT investments.
One insight emerging from BMC’s analytics work was that certain inpatients needed rehabilitation care, which was expensive to provide within a hospital and could be better delivered by dedicated rehab centers.
Moving these patients to outside facilities, however, was not easy: BMC’s position as a safety-net hospital in Boston meant that many of the people it served lacked insurance to cover rehabilitation care.
Nonetheless, it was clear that keeping a rehab candidate in a hospital bed was not only suboptimal in terms of the patient’s health; it also limited BMC’s ability to admit other individuals needing inpatient beds.
Accordingly, the hospital decided to pay the costs of treating uncovered patients in an outside rehabilitation facility.
That benefited everyone: Rehab patients got more-appropriate care, and the hospital’s incurred costs were exceeded by the revenue from additional acute-care patients.
The change in BMC’s business model for rehabilitation patients is part of a broader shift in the United States away from the predominant fee-for-service model (under which clinicians get paid only when they see a patient for an office visit, a hospital admission, a test, or a procedure) and toward a value-based payment system that awards health care organizations a fixed fee per patient for a specified period or care episode.
Both public and private payers are involved in this transformation.
A well-functioning IT system that equips clinicians to improve the quality of their care and to understand and control their costs enables them to be proactive in accepting-even proposing-such arrangements with payers.
For example, Intermountain’s sophisticated IT system has played a major role in its development of a population-based business model that relies on value-based reimbursement. (See “The Case for Capitation,” HBR, July-August 2016.)
One element of its model is its SelectHealth Share insurance plan, which offers large employers a three-year contract that limits premium increases to the consumer price index plus one percentage point a year-significantly below historic increases.
As a greater proportion of its patient base shifts into models like this, Intermountain will be motivated to draw further on its substantial investments in IT, data analytics, protocol development, and workflow changes to improve the quality and lower the cost of its care delivery.
CONCLUSION
Policymakers and economists talk constantly about “bending the cost curve” in health care-turning a bloated, wasteful system that is growing more rapidly than the economy into one that spends much less and grows at a slower pace.
We have seen IT bend the cost curve in many other industries.
Our research suggests that the same can be true in health care, and there are pockets of success to point to. But the necessary work is only just beginning.
Big problems in IT infrastructure must be overcome. Many of today’s systems are too rigid: It’s not easy to customize them, enter and extract information, or continuously update them to incorporate new clinical protocols.
Furthermore, different systems can’t readily share information, making it difficult to create a health record that contains a patient’s full medical history and is accessible to any clinician in any health care organization.
The lack of information sharing is also an obstacle to pooling the huge amounts of anonymized patient data required to find new ways to treat diseases.
In addition to tackling these technological challenges, leaders of many health care organizations will have to do what their progressive peers have done: revamp so that they can use IT to produce better patient outcomes at a lower cost.
The hurdles keeping organizations from harnessing their IT systems to transform health care are surmountable.
What’s needed most is the will and support of an organization’s leaders and clinicians.
A version of this article appeared in the November-December 2017 issue (p.128–138) of Harvard Business Review.
Originally published at https://hbr.org on November 1, 2017.







