Ongoing transmission between vaccinated people makes it essential for those who remain unvaccinated to get the vaccine, especially as more people spend time indoors during the winter months.
JAMA Network
Bridget M. Kuehn, MSJ
December 21, 2021
JAMA. 2021;326(23):2353. doi:10.1001/jama.2021.22316
newsmedial
Being fully vaccinated against SARS-CoV-2 makes it less likely but far from impossible to become infected when another member of the household has a highly transmissible Delta variant infection, according to a study in the United Kingdom.
Altogether, the study enrolled 621 participants: 440 household contacts and 162 nonhousehold contacts of people with SARS-CoV-2 infection as well as 19 index cases.
Among the contacts, 369 were recruited for the study between mid-September 2020 and mid-March 2021 when the Alpha variant predominated in London.
Another group of 233 contacts and the 19 index cases were recruited between late May and mid-September 2021 after the Delta variant emerged.
Contacts collected daily nasal swab samples for up to 20 days and submitted them for diagnostic reverse transcriptase–polymerase chain reaction testing.
Epidemiologic analysis showed that 25% of fully vaccinated individuals who were exposed to the Delta variant through household contact became infected compared with 38% of unvaccinated individuals.
The vaccine was 34% effective against the Delta variant — substantially lower than the 40% to 50% effectiveness against household transmission reported before the variant became widespread
Vaccination status among index cases didn’t change the likelihood of household transmission.
lthough the peak viral load was similar among participants regardless of their vaccination status or variant, viral load decreased faster among those who were vaccinated.
Susceptibility to infection increased as early as 2 to 3 months after vaccination.
Co-lead researcher Ajit Lalvani, DM, chair of infectious diseases at Imperial College London, said in a statement that ongoing transmission between vaccinated people makes it essential for those who remain unvaccinated to get the vaccine, especially as more people spend time indoors during the winter months.
ongoing transmission between vaccinated people makes it essential for those who remain unvaccinated to get the vaccine, especially as more people spend time indoors during the winter months.
Originally published at https://jamanetwork.com
ORIGINAL PUBLICATION
Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: a prospective, longitudinal, cohort study
Anika Singanayagam, PhD *
Seran Hakki, PhD *
Jake Dunning, PhD *
Kieran J Madon, MSc
Michael A Crone, MBBCh
Aleksandra Koycheva, BSc
et al.
Open AccessPublished:October 29, 2021
SUMMARY
Background
The SARS-CoV-2 delta (B.1.617.2) variant is highly transmissible and spreading globally, including in populations with high vaccination rates. We aimed to investigate transmission and viral load kinetics in vaccinated and unvaccinated individuals with mild delta variant infection in the community.
Methods
Between Sept 13, 2020, and Sept 15, 2021, 602 community contacts (identified via the UK contract-tracing system) of 471 UK COVID-19 index cases were recruited to the Assessment of Transmission and Contagiousness of COVID-19 in Contacts cohort study and contributed 8145 upper respiratory tract samples from daily sampling for up to 20 days. Household and non-household exposed contacts aged 5 years or older were eligible for recruitment if they could provide informed consent and agree to self-swabbing of the upper respiratory tract. We analysed transmission risk by vaccination status for 231 contacts exposed to 162 epidemiologically linked delta variant-infected index cases. We compared viral load trajectories from fully vaccinated individuals with delta infection (n=29) with unvaccinated individuals with delta (n=16), alpha (B.1.1.7; n=39), and pre-alpha (n=49) infections. Primary outcomes for the epidemiological analysis were to assess the secondary attack rate (SAR) in household contacts stratified by contact vaccination status and the index cases’ vaccination status. Primary outcomes for the viral load kinetics analysis were to detect differences in the peak viral load, viral growth rate, and viral decline rate between participants according to SARS-CoV-2 variant and vaccination status.
Findings
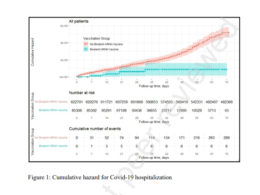
The SAR in household contacts exposed to the delta variant was 25% (95% CI 18–33) for fully vaccinated individuals compared with 38% (24–53) in unvaccinated individuals. The median time between second vaccine dose and study recruitment in fully vaccinated contacts was longer for infected individuals (median 101 days [IQR 74–120]) than for uninfected individuals (64 days [32–97], p=0·001). SAR among household contacts exposed to fully vaccinated index cases was similar to household contacts exposed to unvaccinated index cases (25% [95% CI 15–35] for vaccinated vs 23% [15–31] for unvaccinated). 12 (39%) of 31 infections in fully vaccinated household contacts arose from fully vaccinated epidemiologically linked index cases, further confirmed by genomic and virological analysis in three index case–contact pairs. Although peak viral load did not differ by vaccination status or variant type, it increased modestly with age (difference of 0·39 [95% credible interval –0·03 to 0·79] in peak log10 viral load per mL between those aged 10 years and 50 years). Fully vaccinated individuals with delta variant infection had a faster (posterior probability >0·84) mean rate of viral load decline (0·95 log10 copies per mL per day) than did unvaccinated individuals with pre-alpha (0·69), alpha (0·82), or delta (0·79) variant infections. Within individuals, faster viral load growth was correlated with higher peak viral load (correlation 0·42 [95% credible interval 0·13 to 0·65]) and slower decline (–0·44 [–0·67 to –0·18]).
Interpretation
Vaccination reduces the risk of delta variant infection and accelerates viral clearance. Nonetheless, fully vaccinated individuals with breakthrough infections have peak viral load similar to unvaccinated cases and can efficiently transmit infection in household settings, including to fully vaccinated contacts. Host–virus interactions early in infection may shape the entire viral trajectory.
Funding
National Institute for Health Research.
Research in context
Evidence before this study
The SARS-CoV-2 delta variant is spreading globally, including in populations with high vaccination coverage. While vaccination remains highly effective at attenuating disease severity and preventing death, vaccine effectiveness against infection is reduced for delta. Determining the extent of transmission from vaccinated delta-infected individuals to their vaccinated contacts is a public health priority. Comparing the upper respiratory tract (URT) viral load kinetics of delta infections with those of other variants gives insight into potential mechanisms for its increased transmissibility. We searched PubMed and medRxiv for articles published between database inception and Sept 20, 2021, using search terms describing “SARS-CoV-2, delta variant, viral load, and transmission”. Two studies longitudinally sampled the URT in vaccinated and unvaccinated delta variant-infected individuals to compare viral load kinetics. In a retrospective study of a cohort of hospitalised patients in Singapore, more rapid viral load decline was found in vaccinated individuals than unvaccinated cases. However, the unvaccinated cases in this study had moderate-to-severe infection, which is known to be associated with prolonged shedding. The second study longitudinally sampled professional USA sports players. Again, clearance of delta viral RNA in vaccinated cases was faster than in unvaccinated cases, but only 8% of unvaccinated cases had delta variant infection, complicating interpretation. Lastly, a report of a single-source nosocomial outbreak of a distinct delta sub-lineage in Vietnamese health-care workers plotted viral load kinetics (without comparison with unvaccinated delta infections) and demonstrated transmission between fully vaccinated health-care workers in the nosocomial setting. The findings might therefore not be generalisable beyond the particular setting and distinct viral sub-lineage investigated.
Added value of this study
The majority of SARS-CoV-2 transmission occurs in households, but transmission between fully vaccinated individuals in this setting has not been shown to date. To ascertain secondary transmission with high sensitivity, we longitudinally followed index cases and their contacts (regardless of symptoms) in the community early after exposure to the delta variant of SARS-CoV-2, performing daily quantitative RT-PCR on URT samples for 14–20 days. We found that the secondary attack rate in fully vaccinated household contacts was high at 25%, but this value was lower than that of unvaccinated contacts (38%). Risk of infection increased with time in the 2–3 months since the second dose of vaccine. The proportion of infected contacts was similar regardless of the index cases’ vaccination status. We observed transmission of the delta variant between fully vaccinated index cases and their fully vaccinated contacts in several households, confirmed by whole-genome sequencing. Peak viral load did not differ by vaccination status or variant type but did increase modestly with age. Vaccinated delta cases experienced faster viral load decline than did unvaccinated alpha or delta cases. Across study participants, faster viral load growth was correlated with higher peak viral load and slower decline, suggesting that host–virus interactions early in infection shape the entire viral trajectory. Since our findings are derived from community household contacts in a real-life setting, they are probably generalisable to the general population.
Implications of all the available evidence
Although vaccines remain highly effective at preventing severe disease and deaths from COVID-19, our findings suggest that vaccination is not sufficient to prevent transmission of the delta variant in household settings with prolonged exposures. Our findings highlight the importance of community studies to characterise the epidemiological phenotype of new SARS-CoV-2 variants in increasingly highly vaccinated populations. Continued public health and social measures to curb transmission of the delta variant remain important, even in vaccinated individuals.