JAMA Network
Rajesh T. Gandhi, MD1; Preeti N. Malani, MD, MSJ2,3; Carlos del Rio, MD4January 14, 2022
Substantial progress has been made in therapeutics for nonhospitalized patients with COVID-19, but supply of and access to treatment remain limited.
This Viewpoint summarizes currently available therapeutics for nonhospitalized patients in the setting of the Omicron variant including principles for equitable allocation.
Patients with mild or moderate COVID-19 are those who have respiratory and systemic symptoms but not hypoxia, tachypnea, or other complications that necessitate hospitalization.1
During this early phase of illness, viral replication is occurring and antiviral therapies are used to prevent disease progression, hospitalization, and death.
Antivirals target different stages of the SARS-CoV-2 life cycle. Anti–SARS-CoV-2 monoclonal antibodies bind to the viral spike protein, preventing attachment and entry into cells. Nirmatrelvir-ritonavir inhibits the SARS-CoV-2 main protease, which cleaves viral polyproteins into nonstructural proteins essential for replication. Molnupiravir and remdesivir target SARS-CoV-2 RNA replication: the former induces RNA mutagenesis leading to virus that is unable to replicate and the latter is a nucleotide prodrug that inhibits viral RNA polymerase. Because of mutations in the viral spike protein of the Omicron variant, most currently available anti–SARS-CoV-2 monoclonal antibodies have reduced activity. Nirmatrelvir-ritonavir, remdesivir, and molnupiravir, which target more conserved viral regions, are expected to remain active against Omicron.
Treatment Options in the Omicron Era
- Sotrovimab.
- Nirmatrelvir-Ritonavir.
- Remdesivir.
- Molnupiravir.
Sotrovimab. Three antispike monoclonal antibody products are currently authorized in the US for treatment of high-risk nonhospitalized patients with mild to moderate COVID-19 who are within 10 days of symptom onset: bamlanivimab plus etesevimab, casirivimab plus imdevimab, and sotrovimab.2
A preliminary non–peer-reviewed laboratory study demonstrated marked reduction in the activity of bamlanivimab/etesevimab and casirivimab/imdevimab against Omicron; by contrast, sotrovimab remained active.3 As a result, the National Institutes of Health (NIH) COVID-19 treatment guidelines recommend that sotrovimab, but not bamlanivimab/etesevimab or casirivimab/imdevimab, be used in areas with a high prevalence of Omicron.4
Nirmatrelvir-Ritonavir. Nirmatrelvir is co-formulated with ritonavir to inhibit CYP3A metabolism of nirmatrelvir and achieve therapeutic levels.5 In a phase 2/3 trial, 2246 nonhospitalized participants with COVID-19 who were at high risk of progression and within 5 days of symptom onset were randomly assigned to receive nirmatrelvir-ritonavir or placebo.6
Participants who received nirmatrelvir-ritonavir had an 88% reduction in hospitalization or death compared with the placebo group: 8 of 1039 (0.8%) vs 66 of 1046 (6.3%).
On December 22, 2021, the US Food and Drug Administration (FDA) issued Emergency Use Authorization of nirmatrelvir-ritonavir for treatment of mild to moderate COVID-19 in adult and pediatric patients (age ≥12 years and ≥40 kg) who are at high risk for progression and within 5 days of symptom onset.
Because ritonavir inhibits CYP3A, it alters the metabolism of many other drugs.
Nirmatrelvir-ritonavir should not be administered with medications such as amiodarone (and several other antiarrhythmic drugs), rifampin, or rivaroxaban.
Other medications, such as calcineurin inhibitors, may need dose reduction or close monitoring. Medications such as statins may be temporarily stopped.
Prior to prescribing nirmatrelvir-ritonavir for patients taking other medications, clinicians should consult with an experienced pharmacist to assess potential drug interactions.
Remdesivir. Remdesivir is FDA approved for treatment of hospitalized patients with COVID-19. In a randomized trial, 562 nonhospitalized patients with COVID-19 who were within 7 days of symptom onset and had at least 1 risk factor for disease progression were randomly assigned to receive intravenous remdesivir or placebo on 3 consecutive days.7
Participants who received remdesivir had a decreased risk of hospitalization compared with the placebo group: 2 of 279 (0.7%) receiving remdesivir and 15 of 283 (5.3%) receiving placebo.
There were no deaths in either group. Based on these results, the NIH and Infectious Diseases Society of America COVID-19 treatment guidelines suggested remdesivir as an option for high-risk, nonhospitalized patients who are within 7 days of symptom onset.4,8 This outpatient use of remdesivir is currently off-label.
Molnupiravir. In a phase 3 trial, 1433 nonhospitalized adults with mild to moderate COVID-19 who had at least 1 risk factor for severe disease and who were within 5 days of symptom onset were randomly assigned to receive molnupiravir or placebo twice daily for 5 days.9
In the final analysis, participants who received molnupiravir had a 30% reduction in hospitalization or death compared with the placebo group (6.8% and 9.7%, respectively). This efficacy was lower than that observed in an interim analysis; the reasons for this difference are not clear.
Because of its mechanism of action, there have been theoretical concerns that molnupiravir may cause mutations in human DNA10 or hasten development of new viral variants.
The FDA concluded that the drug has a “low risk for genotoxicity” but is requiring the manufacturer to develop a process to evaluate genomic databases for new viral variants.
On December 23, 2021, the FDA issued an Emergency Use Authorization for molnupiravir for treatment of adults with mild to moderate COVID-19 who are at high risk for progression and within 5 days of symptom onset but only if other authorized therapeutic options are not “accessible or clinically appropriate.”
Molnupiravir is not recommended during pregnancy and is not authorized for children. The FDA recommends that individuals of child-bearing potential should use contraception during treatment and for 4 days after the last dose, and that males of reproductive potential who are sexually active with females of child-bearing potential should use contraception during treatment and for at least 3 months after the last dose.
How Do Outpatient Therapies Compare?
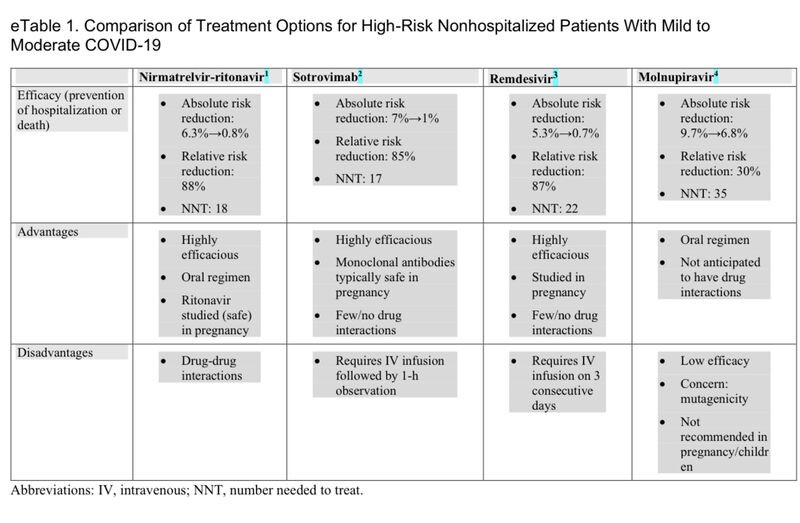
Each of the new therapies has potential advantages and disadvantages (eTable 1 in the Supplement).
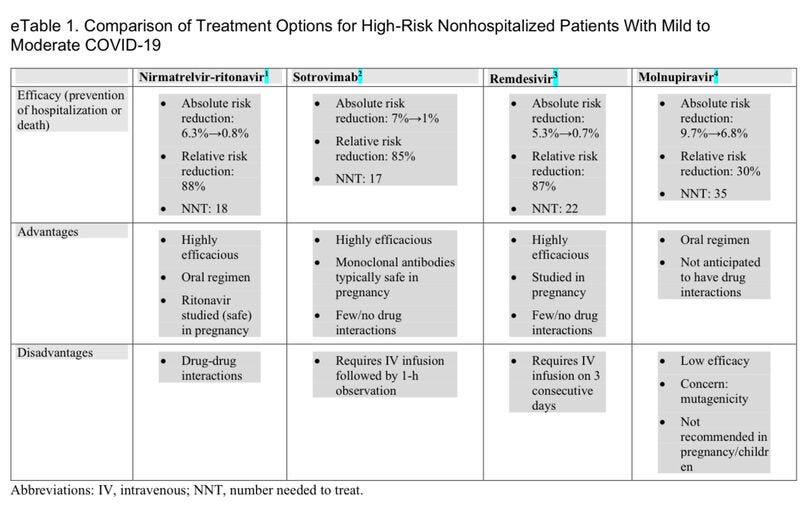
For most individuals, nirmatrelvir-ritonavir will be preferred because of its higher efficacy and the convenience of oral dosing (eTable 2 in the Supplement).
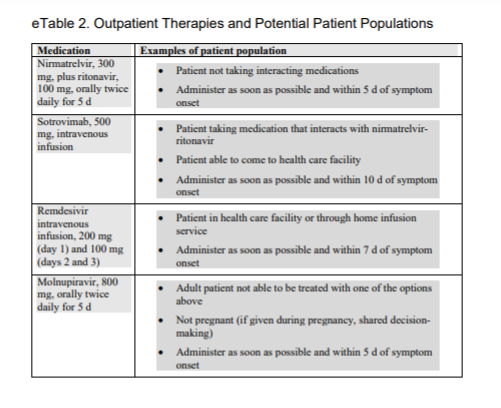
However, there will be circumstances in which nirmatrelvir-ritonavir should not be used because of serious drug interactions. In these patients, sotrovimab would be the preferred choice.
If sotrovimab is not available, then remdesivir is a reasonable next option. The major advantage of remdesivir is a greater supply of the drug at this time; the main disadvantage is the need for intravenous infusion on 3 consecutive days.
Remdesivir is particularly well-suited for use in a patient who is already in a health care setting, such as a skilled nursing facility, or in a person for whom home infusion services can be arranged.
If none of the other options are accessible or appropriate, molnupiravir may be prescribed with the cautions summarized above.
Treatment for Children and Pregnant People
Remdesivir has been used during pregnancy and no safety concerns have emerged. Monoclonal antibodies are generally considered safe during pregnancy.
There are no data on nirmatrelvir during pregnancy, but ritonavir (its pharmacologic booster) is considered safe based on extensive use as a treatment for HIV.
Molnupiravir is not recommended during pregnancy.
Nirmatrelvir-ritonavir and sotrovimab are authorized for children 12 years and older who weigh 40 kg or more.
Remdesivir is approved for treatment of hospitalized children 12 years and older who weigh 40 kg or more and is authorized for treatment of hospitalized children younger than 12 years who weigh at least 3.5 kg. Molnupiravir should not be used in children.
Allocating Treatments When Demand Exceeds Supply
Because the current supply of outpatient treatment options is greatly exceeded by demand, how should clinicians and health care systems maximize benefits of the new medications?
Patients at highest risk for severe disease should be prioritized.
The NIH COVID-19 treatment guidelines have proposed a prioritization scheme for when there are logistical or supply constraints.4
When the number of patients in the highest risk tier exceeds medication supplies, other approaches such as lotteries may be needed.
The distribution of medications should be actively monitored and adjusted to ensure equitable use (ie, vulnerable and disadvantaged individuals are not being excluded).
When supply constraints eventually ease, the treatments should be expanded to a broader population.
Future Directions
Major questions still need to be answered to optimize COVID-19 treatment for nonhospitalized patients.
What is the benefit of therapies in lower-risk patients, such as those who have breakthrough infection after vaccination?
The studies summarized here were conducted in unvaccinated individuals before the emergence of the Omicron variant.
It is likely that the benefit of treatment is lower among patients who are not at high risk for progression to severe disease.
What is the role of combination therapy?
To date, therapies have been evaluated as single agents, and there is concern that viral resistance may emerge, particularly among severely immunosuppressed patients who may have prolonged SARS-CoV-2 replication.
Monitoring for the emergence of resistance among patients receiving monotherapies is needed along with trials to evaluate antiviral combinations. Does treatment of SARS-CoV-2 prevent transmission and does early therapy reduce postacute sequelae of SARS-CoV-2 infection?
Because antiviral therapies are most effective when used early, access to SARS-CoV-2 testing must be expanded along with systems to rapidly offer treatment.
In addition, equitable distribution of these life-saving medications must be ensured, not just in wealthy countries but throughout the world.
The need for a global approach is evident for vaccines, but should also be for diagnostics and therapeutics.
Infections with global morbidity and mortality must be addressed with a coordinated global response.
This principle must be applied to COVID-19 but also to future pandemic strategies that are proactive, evidence-based, and guided by a focus on interconnectedness, equity, and justice.
About the authors & affiliations
Rajesh T. Gandhi, MD1; Preeti N. Malani, MD, MSJ2,3; Carlos del Rio, MD4
1 Massachusetts General Hospital, Harvard Medical School, Boston
2 Division of Infectious Diseases, Department of Internal Medicine, University of Michigan Health System, Ann Arbor
3 Associate Editor, JAMA
4 Division of Infectious Diseases, Department of Medicine, Emory University School of Medicine, Georgia Grady Health System, Atlanta, Georgia
References
See original publication
Originally published at https://jamanetwork.com