Some studies suggest that the risk of cardiovascular problems, such as a heart attack or stroke, remains high even many months after a SARS-CoV-2 infection clears up.
Researchers are starting to pin down the frequency of these issues and what is causing the damage.
Nature
Saima May Sidik
02 August 2022
Executive Summary by:
Joaquim Cardoso MSc
health transformation institute (HTI)
October 17, 2022
In one study this year, researchers used records from the US Department of Veterans Affairs (VA) to estimate how often COVID-19 leads to cardiovascular problems.
- They found that people who had had the disease faced substantially increased risks for 20 cardiovascular conditions — including potentially catastrophic problems such as heart attacks and strokes — in the year after infection with the coronavirus SARS-CoV-2.
- Researchers say that these complications can happen even in people who seem to have completely recovered from a mild infection.
Some smaller studies have mirrored these findings, but others find lower rates of complications.
With millions or perhaps even billions of people having been infected with SARS-CoV-2, clinicians are wondering whether the pandemic will be followed by a cardiovascular aftershock.
- Meanwhile, researchers are trying to understand who is most at risk of these heart-related problems, how long the risk persists and what causes these symptoms.
- It’s a gaping hole in an important area of public health
Here, Nature looks at the questions that scientists are asking and the answers they’ve uncovered so far.
Infographic
ORIGINAL PUBLICATION
Some studies suggest that the risk of cardiovascular problems, such as a heart attack or stroke, remains high even many months after a SARS-CoV-2 infection clears up.
Researchers are starting to pin down the frequency of these issues and what is causing the damage.
In December 2020, a week before cardiologist Stuart Katz was scheduled to receive his first COVID-19 vaccine, he came down with a fever.
He spent the next two weeks wracked with a cough, body aches and chills. After months of helping others to weather the pandemic, Katz, who works at New York University, was having his own first-hand experience of COVID-19.
On Christmas Day, Katz’s acute illness finally subsided. But many symptoms lingered, including some related to the organ he’s built his career around: the heart.
Walking up two flights of stairs would leave him breathless, with his heart racing at 120 beats per minute. Over the next several months, he began to feel better, and he’s now back to his normal routine of walking and cycling. But reports about COVID-19’s effects on the cardiovascular system have made him concerned about his long-term health. “I say to myself, ‘Well, is it really over?’” Katz says.
In one study this year, researchers used records from the US Department of Veterans Affairs (VA) to estimate how often COVID-19 leads to cardiovascular problems.
They found that people who had had the disease faced substantially increased risks for 20 cardiovascular conditions — including potentially catastrophic problems such as heart attacks and strokes — in the year after infection with the coronavirus SARS-CoV-2.
Researchers say that these complications can happen even in people who seem to have completely recovered from a mild infection.
Some smaller studies have mirrored these findings, but others find lower rates of complications.
With millions or perhaps even billions of people having been infected with SARS-CoV-2, clinicians are wondering whether the pandemic will be followed by a cardiovascular aftershock.
With millions or perhaps even billions of people having been infected with SARS-CoV-2, clinicians are wondering whether the pandemic will be followed by a cardiovascular aftershock.
Meanwhile, researchers are trying to understand who is most at risk of these heart-related problems, how long the risk persists and what causes these symptoms.
It’s a gaping hole in an important area of public health, says Katz.
“We don’t understand if this changes the lifelong trajectory for risk of a heart attack or stroke or other cardiac events — we just don’t know that.”
It’s a gaping hole in an important area of public health, says Katz.
“We don’t understand if this changes the lifelong trajectory for risk of a heart attack or stroke or other cardiac events — we just don’t know that.”
Here, Nature looks at the questions that scientists are asking and the answers they’ve uncovered so far.
How many people are at risk?
Doctors have reported cardiovascular problems related to COVID-19 throughout the pandemic, but concerns over this issue surged after the results of the VA study came out earlier this year.
The analysis by Ziyad Al-Aly, an epidemiologist at Washington University in St. Louis, Missouri, and his colleagues is one of the most extensive efforts to characterize what happens to the heart and circulatory system after the acute phase of COVID-19.
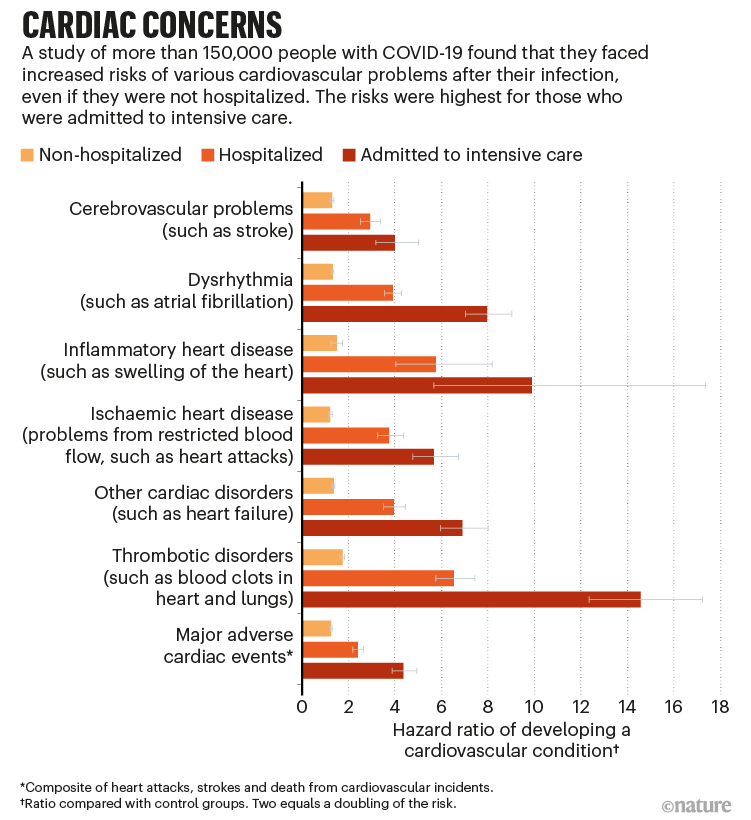
The researchers compared more than 150,000 veterans who had recovered from acute COVID-19 with their uninfected peers, as well as with a pre-pandemic control group.
People who had been admitted to intensive care with acute infections had a drastically higher risk of cardiovascular problems during the next year (see ‘Cardiac concerns’).
For some conditions, such as swelling of the heart and blood clots in the lungs, the risk shot up at least 20-fold compared with that in uninfected peers.
But even people who had not been hospitalized had increased risks of many conditions, ranging from an 8% increase in the rate of heart attacks to a 247% increase in the rate of heart inflammation.
For Al-Aly, the study added to the growing body of evidence that a bout of COVID-19 can permanently alter some people’s health.
These kinds of change fall under the category of post-acute sequelae of COVID-19, which covers problems that emerge after an initial infection.
This disorder includes — and overlaps with — the persistent condition known as long COVID, a term that has many definitions.
These kinds of change fall under the category of post-acute sequelae of COVID-19, which covers problems that emerge after an initial infection.
This disorder includes — and overlaps with — the persistent condition known as long COVID, a term that has many definitions.
Studies indicate that the coronavirus is associated with a wide range of lasting problems, such as diabetes, persistent lung damage and even brain damage.
As with these conditions, Al-Aly says that the cardiovascular issues that occur after a SARS-CoV-2 infection can decrease a person’s quality of life over the long term.
Treatments do exist for these problems, “but they are not curable conditions”, he adds.
Studies indicate that the coronavirus is associated with a wide range of lasting problems, such as diabetes, persistent lung damage and even brain damage.
… the cardiovascular issues that occur after a SARS-CoV-2 infection can decrease a person’s quality of life over the long term.
Despite its large size, the VA study does come with caveats, say researchers.
The study is observational, meaning that it reuses data that were collected for other purposes — a method that can introduce biases.
For example, the study considers only veterans, meaning that the data are skewed towards white men.
“We don’t really have any study like it that goes into more diverse and a younger population,” says Eric Topol, a genomicist at Scripps Research in La Jolla, California.
He thinks that more research is needed before scientists can truly quantify the frequency at which cardiovascular problems strike.
… more research is needed before scientists can truly quantify the frequency at which cardiovascular problems strike.
Daniel Tancredi, a medical statistician at the University of California, Davis, points out another potential source of bias.
One of the control groups in the VA study had to get through more than a year without catching SARS-CoV-2 to be included in the study.
There could be physiological differences that made the control group less likely to contract the disease, which could also affect their susceptibility to cardiovascular problems.
Still, Tancredi thinks the study was well designed and that any bias is likely to be minimal.
“I wouldn’t say that these numbers are exactly right, but they’re definitely in the ballpark,” he says.
He hopes future prospective studies will fine-tune Al-Aly’s estimates.
Some other studies do point in the same direction.
Data from the England’s health-care system, for example, show that people who had been hospitalized with COVID-19 were about three times more likely than uninfected people to face major cardiovascular problems within eight months of their hospitalization.
Data from the England’s health-care system, for example, show that people who had been hospitalized with COVID-19 were about three times more likely than uninfected people to face major cardiovascular problems within eight months of their hospitalization.
A second study found that, in the 4 months after infection, people who had had COVID-19 had a roughly 2.5-fold increased risk of congestive heart failure compared with those who had not been infected.
Health modeller Sarah Wulf Hanson at the University of Washington’s Institute for Health Metrics and Evaluation in Seattle used Al-Aly’s data to estimate how many heart attacks and strokes COVID-19 has been associated with.
Her unpublished work suggests that, in 2020, complications after COVID-19 caused 12,000 extra strokes and 44,000 extra heart attacks in the United States, numbers that jumped up to 18,000 strokes and 66,000 heart attacks in 2021.
This means that COVID-19 could have increased the rates of heart attack by about 8% and of stroke by about 2%. “It is sobering,” Wulf Hanson says.
This means that COVID-19 could have increased the rates of heart attack by about 8% and of stroke by about 2%. “It is sobering,” Wulf Hanson says.
Indirect effects of the COVID-19 pandemic, such as missed medical appointments, stress and the sedentary nature of isolating at home probably further contributed to the cardiovascular burden for many people, scientists suggest.
Indirect effects of the COVID-19 pandemic, such as missed medical appointments, stress and the sedentary nature of isolating at home probably further contributed to the cardiovascular burden for many people, scientists suggest.
These numbers don’t match what some researchers have seen in the clinic, however.
In a small study of 52 people, Gerry McCann, a cardiac-imaging specialist at the University of Leicester, UK, and his colleagues found that …
… people who had recovered after being hospitalized with COVID-19 had no greater rate of heart disease than did a group of people who had similar underlying conditions but remained uninfected.
The trial was orders of magnitude smaller than Al-Aly’s, but McCann and his colleagues are working on a larger study with around 1,200 participants.
The results have yet to be published, but McCann says “the more data we’re acquiring, the less impressed we are with the degree of, let’s say, myocardial injury”, or heart problems.
The results [from the small UK study] have yet to be published, but McCann says “the more data we’re acquiring, the less impressed we are with the degree of, let’s say, myocardial injury”, or heart problems.
Despite having an incomplete picture of COVID-19’s cardiovascular effects, doctors recommend caution.
An expert panel convened by the American College of Cardiology advises doctors to test people who have had COVID-19 for cardiovascular problems if they have risk factors such as being older or immunosuppressed.
Despite having an incomplete picture of COVID-19’s cardiovascular effects, doctors recommend caution.
An expert panel convened by the American College of Cardiology advises doctors to test people who have had COVID-19 for cardiovascular problems if they have risk factors such as being older or immunosuppressed.
Despite having an incomplete picture of COVID-19’s cardiovascular effects, doctors recommend caution.
An expert panel convened by the American College of Cardiology advises doctors to test people who have had COVID-19 for cardiovascular problems if they have risk factors such as being older or immunosuppressed.
How are researchers gathering more information?
Answers to many questions about the long-term impacts of COVID-19 could come from a large study called the Researching COVID to Enhance Recovery, or RECOVER, project, …
… which aims to follow 60,000 people for up to 4 years at more than 200 sites in the United States.
The study will include participants with long COVID, people who were infected and have recovered, and others who were never infected.
“It’s enrolling across the lifespan,” says Katz, who is the principal investigator of the trial. He and his colleagues plan to study children, adults, pregnant people and the infants who are born during the trial.
Most RECOVER participants will fill out questionnaires about their health and undergo non-invasive tests.
Researchers aim to collect extra information for about 20% of participants, for example, by temporarily inserting small tubes into adults’ hearts to obtain localized measurements of indicators such as blood pressure and oxygen levels.
After several years, scientists hope to have completed a catalogue of long-COVID symptoms, formed an understanding of who develops them and begun to understand why they occur.
In the United Kingdom, McCann leads the cardiovascular working group for a similar project called the Post-hospitalization COVID-19 study, or PHOSP-COVID.
This multi-centre study focuses on people who were hospitalized with COVID-19, and aims to uncover the prevalence of lasting symptoms, who is most at risk and how the virus causes lingering health problems.
Thus far, the group has found that only about one-quarter of people who were hospitalized feel fully recovered one year after infection.
And the team has identified immune markers that are associated with the worst cases of long COVID.
How does the virus harm the heart?
COVID-19’s effect on the heart could be related to the key protein that the virus uses to enter cells.
It binds to a protein called ACE2, which can be found on the surfaces of dozens of types of human cell. This, says Al-Aly, gives it “access and permission to enter almost any cell in the body”.
When the virus enters the endothelial cells that line blood vessels, Topol says, that’s probably where many cardiovascular problems start.
Blood clots form naturally to heal damage caused while the body clears the infection. These clots can clog blood vessels, leading to damage as minor as leg pain or as severe as a heart attack.
A study based on more than 500,000 COVID-19 cases found that people who had been infected had a 167% higher risk of developing a blood clot in the two weeks after infection than people who had had influenza.
A study based on more than 500,000 COVID-19 cases found that people who had been infected had a 167% higher risk of developing a blood clot in the two weeks after infection than people who had had influenza.
Robert Harrington, a cardiologist at Stanford University in California, says that even after the initial infection, plaques can accumulate where the immune response has damaged the lining of blood vessels, causing the vessels to narrow.
This can lead to problems, such as heart attacks and strokes, even months after the initial wound has healed.
“Those early complications can definitely translate into later complications,” Harrington says.
… even after the initial infection, plaques can accumulate where the immune response has damaged the lining of blood vessels, causing the vessels to narrow. This can lead to problems, such as heart attacks and strokes, even months after the initial wound has healed.
SARS-CoV-2 could also leave its fingerprints on the immune system.
When Akiko Iwasaki, an immunologist at Yale University in New Haven, Connecticut, and her colleagues characterized antibodies from hospitalized people during the acute phase of COVID-19, they found a plethora of antibodies against human tissue.
SARS-CoV-2 could also leave its fingerprints on the immune system. When scientists characterized antibodies from hospitalized people during the acute phase of COVID-19, they found a plethora of antibodies against human tissue.
Iwasaki suspects that when SARS-CoV-2 ramps up someone’s immune system, it might inadvertently activate immune cells that attack the body — cells that stay quiet when the immune system isn’t in overdrive.
These immune cells could damage many organs, including the heart.
Damage to blood vessels can compound attacks on the immune system.
“You can think of this damage as accumulating over time,” says Iwasaki.
When the cardiovascular system has been assaulted on enough fronts, that’s when people can experience serious consequences, such as a stroke or heart attack.
Damage to blood vessels can compound attacks on the immune system. “You can think of this damage as accumulating over time,”
When the cardiovascular system has been assaulted on enough fronts, that’s when people can experience serious consequences, such as a stroke or heart attack.
What about reinfection and new variants?
Vaccinations, reinfections and the Omicron variant of SARS-CoV-2 all pose new questions about the virus’s cardiovascular effects.
A paper published in May by Al-Aly and his colleagues suggests that vaccination reduces, but does not eliminate, the risk of developing these long-term problems.
… vaccination reduces, but does not eliminate, the risk of developing these long-term problems.
Hanson is also eager to model whether reinfections compound the risk and whether the relatively mild — but widespread — Omicron variant will affect the cardiovascular system as drastically as other variants.
“We are kind of chomping at the bit for follow-up data among Omicron cases,” she says.
Originally published at https://www.nature.com on August 2, 2022.
Names mentioned
Ziyad Al-Aly, an epidemiologist at Washington University in St. Louis, Missouri,
Eric Topol, a genomicist at Scripps Research in La Jolla, California.
Daniel Tancredi, a medical statistician at the University of California, Davis,
Health modeller Sarah Wulf Hanson at the University of Washington’s Institute for Health Metrics and Evaluation in Seattle
Gerry McCann, a cardiac-imaging specialist at the University of Leicester, UK
American College of Cardiology
Robert Harrington, a cardiologist at Stanford University in California
Akiko Iwasaki, an immunologist at Yale University in New Haven, Connecticut