HealthSystems — transformation institute
Joaquim Cardoso MSc
Chief Researcher, Editor and Strategy Officer (CSO)
November 15, 2022
Executive Summary
What is the context?
- The Telehealth momentum after the pandemic was short-lived:
– only 29% of Medicaid and Medicare users had at least one telehealth visit throughout the first quarter of 2022, according to the most recent Centers for Medicare & Medicaid Services data,
– down from 46% in all of 2021.
What happened to healthcare’s darling technology of the moment?
- Time and place. Healthcare is — and will always be — highly personal.
- While virtual care has proved to be a critical tool for creating access, especially for urgent and mental health care, it is just that — one tool.
- The reality is that many people still want in-person care options.
- At the end of the day, no piece of technology will ever compare to the physical touch of a clinician.
What is telehealth?
- Telehealth is a tool, not a toolbox
- It is remarkably easy to get caught up in the hype of a technology and its potential impact and forget about the person who simply expects convenient access to a clinician they know and trust.
- At Livongo, we took an important step by using data and machine learning to deliver personalized insights, coaching, and emergency outreach when someone was at risk for an acute hypoglycemic event.
What telehealth can not provide, alone?
- But Livongo, like Castlight, was missing human touch.
- Human touch remains the single most important ingredient in creating trust between a person and their clinician, and the reason why technology solutions themselves will never be able to stand alone in the service of patient-provider relationships.
- In order to build trust, there has to be a personal touch at some point in everyone’s healthcare journey.
- People want more face time with clinicians they know and love.
Who is doing it?
- This is why service-dominant care models like One Medical and Oak Street Health have been able to sustain interest prior to and beyond the COVID-19 pandemic.
- They understand virtual care is but one tool in the care delivery toolbox, and when clinicians are in close proximity to the people they treat, it is often not the tool patients prefer.
- It’s why ChenMed providers spend an average of three hours with each patient every year.
What is the issue?
- Increasing the amount of time people spend with their clinician isn’t sustainable in every community.
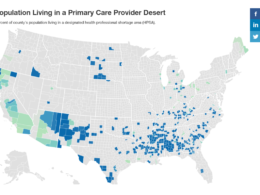
- The U.S. is experiencing a dire provider shortage, and the shortfall is only expected to intensify over the next decade. This provider desert is especially vast in rural communities, where the nearest clinician is often many miles away.
- Service-dominant models can’t solve the issue of access to quality care in rural America, nor can telehealth alone.
What is the solution? The case for hybrid models
- In healthcare, hybrid models borrow the best aspects of technology combined with in-person care, provided directly to patients in their homes and communities.
- Providing convenient access to personal touch is the biggest challenge in clinician-sparse rural communities, where the patient-to-primary care ratio is only 39 physicians per 100,000 people and the patient-to-specialist ratio is even worse. Hospital closures and retirement have left many small towns devoid of practicing medical professionals.
How the model works?
- In communities where access is limited, a hybrid model can deliver comprehensive care, but that care must lead with in-home services.
- Virtual care can be a powerful tool for creating convenience and access, but in-home visits must lay the foundation of trust and clinical insight necessary to make it work in the long term.
- That is the power of hybrid care and the modern-day house call: it starts and continues with the physical touch of a clinician, but is sustained through technology.
ORIGINAL PUBLICATION (full version)

Telehealth is dead. The era of hybrid care has arrived
Fierce Healthcare
By Jennifer Schneider, M.D.
Nov 9, 2022
Healthcare innovation, like anything else, is about time and place.
The technologies we develop to deliver a better and more effective healthcare experience can only be successful if they meet people’s expectations for their care at exactly the moment they need it.
For telehealth, that moment was COVID-19. That moment has passed.
Widespread virtual care adoption in 2020 was critical to keeping people connected to their doctors during a time when access to care was severely limited.
A friendly regulatory environment was cultivated out of necessity, adoption spiked as a result, and investment in telehealth was flowing freely.
Momentum, however, was short-lived: only 29% of Medicaid and Medicare users had at least one telehealth visit throughout the first quarter of 2022, according to the most recent Centers for Medicare & Medicaid Services data, down from 46% in all of 2021.
Momentum, however, was short-lived: only 29% of Medicaid and Medicare users had at least one telehealth visit throughout the first quarter of 2022, according to the most recent Centers for Medicare & Medicaid Services data, down from 46% in all of 2021.
What happened to healthcare’s darling technology of the moment?
Time and place. Healthcare is — and will always be — highly personal.
While virtual care has proved to be a critical tool for creating access, especially for urgent and mental health care, it is just that — one tool.
While virtual care has proved to be a critical tool for creating access, especially for urgent and mental health care, it is just that — one tool.
The reality is that many people still want in-person care options.
At the end of the day, no piece of technology will ever compare to the physical touch of a clinician.
The reality is that many people still want in-person care options. At the end of the day, no piece of technology will ever compare to the physical touch of a clinician.
Telehealth is a tool, not a toolbox
It is remarkably easy to get caught up in the hype of a technology and its potential impact and forget about the person who simply expects convenient access to a clinician they know and trust.
During my time at Castlight, the focus of our work was on creating technology that allowed for people to be educated consumers of healthcare.
When I was president of Livongo, we took an important step by using data and machine learning to deliver personalized insights, coaching, and emergency outreach when someone was at risk for an acute hypoglycemic event.
We got about as close to building a formative relationship between healthcare consumers and providers as was possible with technology alone.
at Livongo, we took an important step by using data and machine learning to deliver personalized insights, coaching, and emergency outreach when someone was at risk for an acute hypoglycemic event.
But Livongo, like Castlight, was missing human touch.
It remains the single most important ingredient in creating trust between a person and their clinician, and the reason why technology solutions themselves will never be able to stand alone in the service of patient-provider relationships.
In order to build trust, there has to be a personal touch at some point in everyone’s healthcare journey.
human touch remains the single most important ingredient in creating trust between a person and their clinician, …
… and the reason why technology solutions themselves will never be able to stand alone in the service of patient-provider relationships.
People want more face time with clinicians they know and love.
This is why service-dominant care models like One Medical and Oak Street Health have been able to sustain interest prior to and beyond the COVID-19 pandemic.
They understand virtual care is but one tool in the care delivery toolbox, and when clinicians are in close proximity to the people they treat, it is often not the tool patients prefer.
It’s why ChenMed providers spend an average of three hours with each patient every year.
People want more face time with clinicians they know and love. This is why service-dominant care models like One Medical and Oak Street Health have been able to sustain interest prior to and beyond the COVID-19 pandemic.
They understand virtual care is but one tool in the care delivery toolbox, and when clinicians are in close proximity to the people they treat, it is often not the tool patients prefer.
However, increasing the amount of time people spend with their clinician isn’t sustainable in every community.
The U.S. is experiencing a dire provider shortage, and the shortfall is only expected to intensify over the next decade. This provider desert is especially vast in rural communities, where the nearest clinician is often many miles away.
Service-dominant models can’t solve the issue of access to quality care in rural America, nor can telehealth alone.
Delivering exceptional care to these communities is not unlike beginning a new business relationship: phone calls and virtual meetings are more comfortable and more effective after you’ve met in person, gotten to know each other, and shaken hands.
In healthcare, hybrid models borrow the best aspects of technology combined with in-person care, provided directly to patients in their homes and communities.
In healthcare, hybrid models borrow the best aspects of technology combined with in-person care, provided directly to patients in their homes and communities.
Providing a personal touch in provider-sparse communities
In medical school, I learned all of the clinical algorithms and regulations needed in order to practice medicine.
What medical school didn’t teach me was the most important part of being a physician: how to put my academic knowledge into practice in the context of care delivery.
When a person walked into my exam room, my job was to encourage them to do whatever was best for their health knowing their lifestyle.
In other words, how do I as a clinician use what I know about a patient as a clinical tool? Simply telling a patient to take a statin pill to lower their low-density lipoprotein, for example, is not motivating. However, if the patient loves deli sandwiches and owns a dog, encouraging the patient to get the exercise they need by taking their dog on a walk to the deli a few times a week will always deliver better results.
We don’t learn that type of tact from a med school textbook.
It is only possible by fostering a trusting, one-to-one relationship with a patient. Virtual interactions don’t typically stimulate this level of relationship-building. People want their clinician to put a hand on their shoulder and listen to what they have to say, to have empathy for their condition, and to help find a solution. It’s a major reason why telehealth hasn’t solved rural healthcare on its own, despite the obvious logistical advantage.
Providing convenient access to personal touch is the biggest challenge in clinician-sparse rural communities, where the patient-to-primary care ratio is only 39 physicians per 100,000 people and the patient-to-specialist ratio is even worse.
Hospital closures and retirement have left many small towns devoid of practicing medical professionals.
Providing convenient access to personal touch is the biggest challenge in clinician-sparse rural communities, where the patient-to-primary care ratio is only 39 physicians per 100,000 people and the patient-to-specialist ratio is even worse.
In communities where access is limited, a hybrid model can deliver comprehensive care, but that care must lead with in-home services.
When a clinician’s first interaction with a new patient takes place in the rich environment of a patient’s home, they are given a window into the lived environment of the person they’re treating. They can see what the patient’s world looks like in context, in a way they wouldn’t be able to determine from clinical data, a ZIP code, a glimpse through a screen, or even in the office.
In communities where access is limited, a hybrid model can deliver comprehensive care, but that care must lead with in-home services.
Virtual care can be a powerful tool for creating convenience and access, but in-home visits must lay the foundation of trust and clinical insight necessary to make it work in the long term.
In the time between in-person and virtual visits, hybrid models should use remote monitoring technology to keep a true, up-to-the-minute pulse on patients. Real-time data collection ensures providers are always connected to their patients, and in urgent cases, can triage care appropriately.
That is the power of hybrid care and the modern-day house call: it starts and continues with the physical touch of a clinician, but is sustained through technology.
That is the power of hybrid care and the modern-day house call: it starts and continues with the physical touch of a clinician, but is sustained through technology.
Digital health has developed powerful, life-changing technologies, but their potential will always be limited if they are deployed without context — context that can only be acquired through a trusting patient-provider relationship. The demand for that relationship will always transcend a moment.
Jennifer Schneider, M.D., is the CEO of Homeward, a technology-enabled healthcare provider delivering care to those who don’t have it, starting in rural America.
Previously, she served five years as the chief medical officer and president of Livongo.
Originally published at https://www.fiercehealthcare.com