US states face the delicate task of scaling back their COVID-19 public-health infrastructure while ensuring that they are better prepared for the next crisis.
BCG
By Lisa Vura-Weis, Michael Choy, Colleen Desmond, Eran Koren, Jonathan Lim, Jonathan Scott, and Selin Zalma
MARCH 11, 2022
In their two-year battle with the coronavirus, US states have reached a delicate moment of transition in their role at the frontline of the pandemic response. The emergency of the Omicron variant appears to be over, but the need for continual vigilance and preparedness remains. Even states with the strictest mask mandates and other public-health interventions are lowering their guard. This is welcome news but should be taken with caution. The US continues to lag other advanced economies in vaccination rates and so remains vulnerable to future outbreaks.
The pandemic harshly exposed gaps in the nation’s decentralized, public-private health care system. It took a lasting toll on the physical and emotional well-being of the health care workforce, engendered lingering distrust across segments of society, and affected historically underserved populations much more severely than other groups.
In this time of relative calm, states have an opportunity to reset the agenda. They can unwind some of their hard testing and vaccination infrastructure while building soft capabilities in preparedness, rapid response, targeted intervention, and communication. They can partner with private health care providers, especially primary-care physicians and pharmacists, to assume a larger role in treatment and prevention, while educating and encouraging residents to behave responsibly given their health status and risk tolerance.
The pandemic was a crisis too valuable to waste. Now is the time to use the lessons of the past two years and prepare for the future. Here are seven priorities.
- Define the Role of the State in Three Postpandemic Scenarios
- Fix the Operating Model
- Invest in the Workforce
- Simplify Communication
- Strengthen Data-Driven Decision Making
- Continue the Focus on Equity and Sharing of Best Practices
- Plan for the Unexpected and the Next Pandemic

1. Define the Role of the State in Three Postpandemic Scenarios
As the Omicron surge recedes, states will play different roles depending on their COVID-19 infection rates and the impact of the disease on their health systems. There are three main scenarios. (See Exhibit 1.)
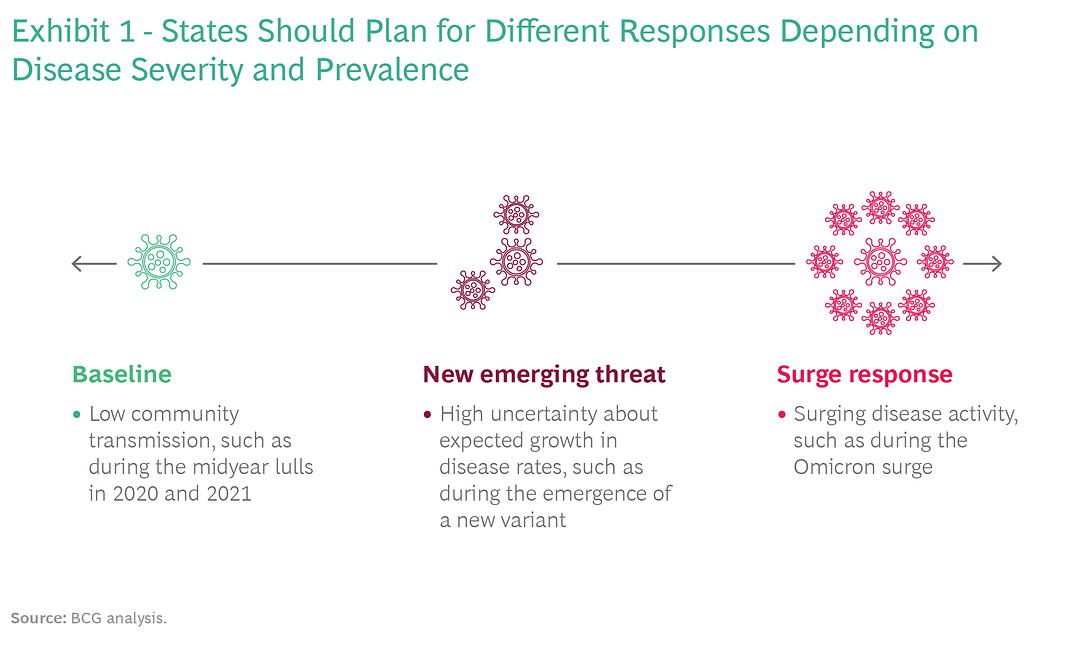
- Baseline: Periods of low to moderate disease with little to manageable impact on the health care system (comparable to the midyear lulls of 2020 and 2021). These periods should be used to enhance preparedness.
- New Emerging Threat: Inflection points when a new variant of concern is identified or a nascent spike in disease activity begins. States should begin increasing surveillance, testing, treatment, and health care system capacity.
- Surge Response: Times when states are experiencing disease activity similar to the Delta or Omicron waves, driven by a variant or by seasonality. States should fully ramp up resources to support the health care system’s responsiveness and resilience.
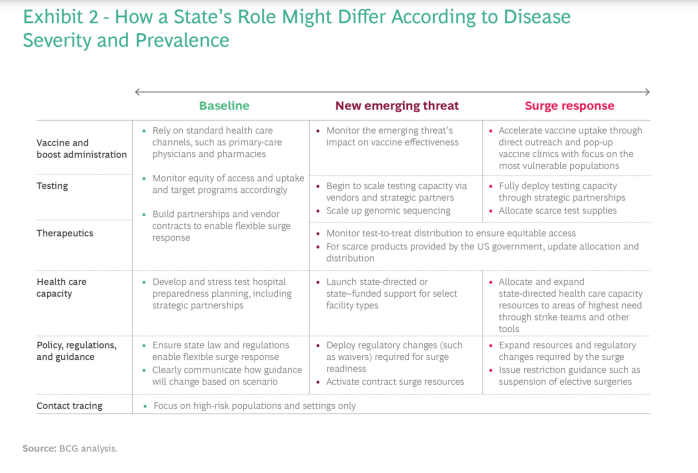
For each of these scenarios, state public-health departments should define and document the role of the state and of private-sector partners in the major categories of pandemic response and management, such as testing and vaccination. Roles will likely vary by population segment and setting. For example, states may want to maintain broad responsibility for vulnerable populations even when cases remain low, or assume more of an advisory role in high-vaccination communities even when cases are high. (For an example of how a state’s roles might change depending on disease prevalence, see Exhibit 2.)
2. Fix the Operating Model
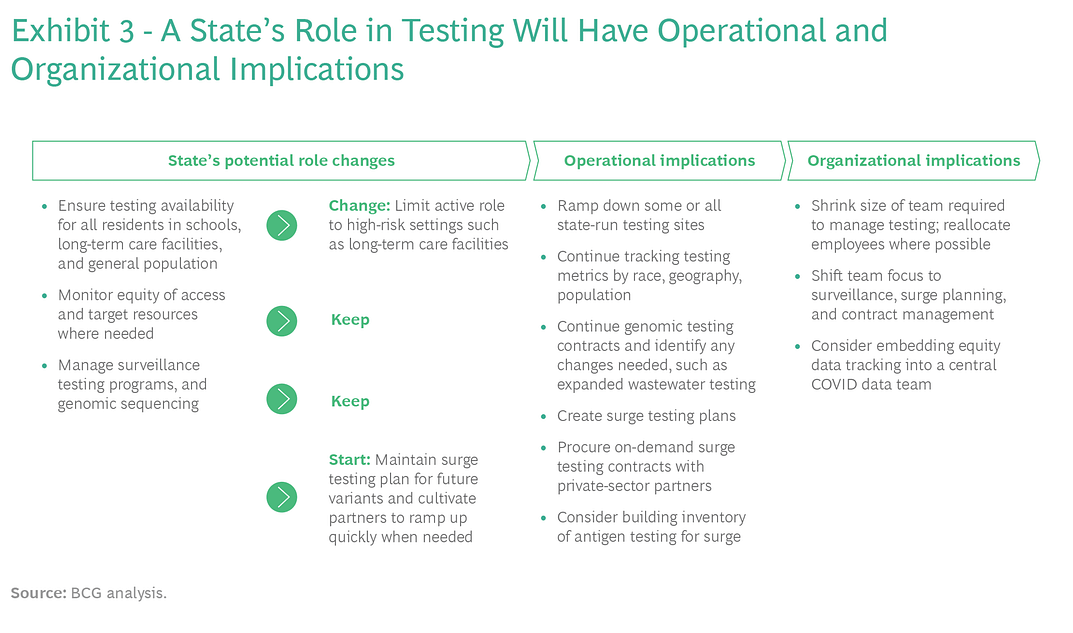
For the past two years, state health departments have engaged in heroic work on the fly. Many of the operational changes implemented are unsustainable. Staff have been reallocated from other public-health programs and large COVID-19 response units have been grafted onto smaller emergency response teams. Now states have the chance to evaluate and properly scope their various programs. One effective way to do this is to conduct a keep/start/change exercise. Certain measures should likely stay in place, such as promotion of vaccines and therapeutics, disease surveillance and reporting, and outbreak investigation and response in high-risk settings. (See Exhibit 3 for an example of how a state’s changed role in testing could affect operations and the public-health system.)
Other responses should be flexible and modular, allowing the health department to handle surges. These include large-scale testing, expanded emergency medical services, and access to direct staffing support for long-term care facilities. Vendors and partners will play a large role in handling surges and coming up with creative solutions, such as “test sites in a box.” New responsibilities will also emerge over time, notably regarding individuals with long COVID. (See “The States’ Role in Long COVID.”)
The keep/start/change exercise should produce answers to a series of fundamental operating and organizational questions:
- Which capabilities and ways of working developed during the pandemic, such as public-private collaboration and streamlined decision making, can be leveraged for other public uses beyond COVID-19?
- What is the best approach to developing data-driven decision making in near real time?
- Which capabilities and teams should be in-house and which capabilities can be handled by vendors, partners, and private providers?
- Should there be an ongoing dedicated COVID team or department? If so, where should it sit, and what solid- and dotted-line reporting should be in place for key functions?
- Would that structure be durable? If it dissolves over time, how and in what sequence would its members be absorbed into the rest of the organization?
3. Invest in the Workforce
The brutal workload and high-intensity demands of the pandemic have taken a heavy toll on the public-health and health care workforce, with a significant loss of experienced talent. States need workforce development strategies for their own health departments as well as for hospitals, long-term-care facilities, and other providers. How can states improve working conditions so that these critical employees remain engaged and productive?
States will play different roles depending on their COVID-19 infection rates and the impact of the disease on their health systems.
Bringing the workforce back to its prepandemic state is a tall order. Creating a resilient and robust workforce able to handle future COVID surges is an even higher bar. In the short run, health departments can consider investing remaining American Rescue Plan Act and other state and federal funds in their state’s health department workforce and in the broader health care workforce. These investments should include mental-health support to mitigate the trauma of the last two years and help retain existing employees. Public-health departments should also consider longer-term sustainable solutions, such as academic partnerships to expand the pipeline of health care workers, loan forgiveness programs, and increases in Medicaid reimbursement rates.
Beyond these fundamental investments, states also need to develop flexibility to ensure that critical workers such as ICU nurses and respiratory therapists are available during any future surges. Many experts believe that COVID-19 hospital admissions and strains in the health care system will emerge next winter and possibly sooner. The current lull is the right time to strengthen partnerships with health care providers and ensure that appropriate resources and planning are dedicated to readiness.
4. Simplify Communications
Public health is moving from a world of mandates and restrictions to one of guidance, individual empowerment, and transparency. During the several peaks of the pandemic, communication often seemed reactive and inconsistent. Public-health departments now have a chance to start anew and develop clear, consistent public messaging about individual risk factors and the actions that people can take to keep their communities safe.
States should develop a communications plan for each of the three scenarios described above. One idea is to create an alert system for COVID-19 similar to what many states already have in place for air pollution and the flu. The past two years have illustrated the different levels of risk that people can tolerate. A key plank of any communications strategy will be providing trustworthy information that lets individuals make decisions based on their specific family, work, and health circumstances, while staying rooted in the best available scientific evidence and risk mitigation guidance.
5. Strengthen Data-Driven Decision Making
The pandemic highlighted many gaps in the public-health data infrastructure. Data collection is inconsistent and often antiquated (with some testing labs still submitting reports via fax). Data validation is often difficult — is this John Doe the same as that John Doe? Legal and policy barriers sometimes constrain data sharing, but often the systems themselves make it difficult to share data easily.
To close these gaps, state health departments should start by modernizing their health data systems and infrastructure. But the issue will not be solved by hardware and software alone. Public-health officials need to update their policy frameworks and data-sharing agreements and upgrade their talent and capabilities. They should also have a flexible approach to data, recognizing when a quick cut of the numbers is adequate for programmatic operations and when definitive statistics and records are necessary. In highly complex environments such as a pandemic or other public-health emergency, officials must become more sophisticated in their use of data to support decision making.
6. Continue the Focus on Equity and Sharing of Best Practices
As the pandemic progressed, states collectively developed increasingly sophisticated data systems to track outcomes across communities and across demographics such as race and income. And yet many gaps remained in vaccination, treatment, and testing rates. States should capture insights from these systems and develop public-health programs focused on equity and fairness. For example, several public-health agencies developed dashboards that tracked vaccination rates by county, race, and age, which helped them target resources to low-vaccination communities and then monitor effectiveness. Unlike previous efforts to track outcomes across communities, these dashboards were updated weekly, allowing for nimble changes to strategy or reallocation of resources. Such an approach could be applied to programs targeting chronic and communicable diseases.
States need workforce development strategies for their own health departments as well as for hospitals, long-term-care facilities, and other providers.
The pandemic also generated innovations in vaccine delivery, such as mobile clinics, free transportation, and partnerships with community groups, all of which could be applied more broadly to reach the underserved.
7. Plan for the Unexpected and the Next Pandemic
COVID has put the spotlight on public health. Next time, the public will expect a speedier and more effective response. States should be building scalable disease surveillance infrastructure so that they can identify and track new COVID-19 variants in the short term. This capability will also allow them to identify and manage emerging diseases in the medium to long term.
To develop game plans, state health departments should run planning exercises based on the three scenarios described above — baseline preparedness, new emerging threat, and surge response — as well as on potential developments at a more granular level. For example, what if PCR tests are unable to detect the next variant? Or the variant affects only certain segments of the population? What if existing vaccines and treatments don’t work at all and a variant-specific vaccine will take months to develop and administer? Whether or not any of these scenarios actually occur, such exercises force leaders to think expansively about the future and the capabilities and preparation that will be needed.
Let’s hope that the worst of COVID-19 is over. But hope is not a strategy.
The best way to prepare for the future is to learn from the past.
And the past two years have given state health departments many lessons relating to preparation, flexibility, resilience, and trust that are too valuable to waste.
Originally published at https://www.bcg.com on March 8, 2022.